
PRESCRIPTION OPIOID
AND HEROIN
AWARENESS TOOLKIT
A PREVENTION GUIDE
PROVIDED BY:

ABOUT GREENBRIER COUNTY
CAR
X
E COALITION
The Greenbrier County Prescription Opioid
& Heroin Awareness Toolkit - Prevention
Guide was originally created by the
Greenbrier County CARxE Coalition, a
substance abuse prevention coalition
under the county’s Family Resource
Network. Planning, oversight and design
development were supported by the West
Virginia School of Osteopathic Medicine
(WVSOM) and facilitated through the
WVSOM Center for Rural and Community
Health. The CARxE Coalition Toolkit
Committee members include:
Molly McMillion
Cheryl Jonese
Debbie Sizemore
Co-Chair Care Coalition, Kim Estep
Co-Chair Care Coalition, Lisa Snedegar
Toolkit Committee Chair, Haylee Heinsberg
Graphic Designer, Jennifer Spencer
The CARxE Substance Abuse Coalition
began in August 2012 at a meeting
with representatives f
rom Greenbrier
Valley Medical Center, Family Resource
Network of Greenbrier County,
United Way of the Greenbrier Valley
and Seneca Health Services. The
discussion centered on the negative
eect the drug epidemic has on the
Greenbrier County area and what
might be done with it. We decided to
host “Community Conversations” with
identied individuals. Our rst meeting
was open to the general public and
more than 65 individuals attended. The
outcome of this meeting was to form
a steering committee that included
all of the above plus our local sheri,
Fritz’s Pharmacy, Greenbrier County
Board of Education, Greenbrier Valley
Chamber of Commerce and Robert C.
Byrd Clinic.
We began hosting “Community
Conversations” with identied groups
such as local law enforcement ocials
and representatives from our faith-
based community. We were also a part
of helping the local Greenbrier County
Health Department with their needs
assessment. Substance abuse was
identied as a top priority issue, which
led the health department to also join
the steering committee.
The steering committee then held
a facilitated discussion to develop
the following mission statement:
“Greenbrier County CARxE Coalition
strives to reduce the eect that
prescription drugs have on our
communities.” This meeting also
included development of a list of
“what we have learned, what we felt
was needed and objectives were also
written.” At that time in 2012, one
of the biggest identied needs was
to work with the WV legislature to
facilitate changes in the WV code to
reduce the availability of drugs and to
increase treatment options.
Currently, we continue to meet with a
lot of new faces. We were presented
with a copy of a “Heroin Toolkit” from
our local United Way who had received
it from another state. Those involved
decided that we should adopt this
format and provide local information
where everything from a listing of local
resources, local stories from survivors
of addiction, signs of substance abuse,
etc. would be found in one place.
REVIEWER
ELEVENTH JUDICIAL
CIRCUIT
Tonya Hoover -
Chief Probation Ocer
SENECA HEALTH SERVICES,
INC. IN GREENBRIER
COUNTY
Jessica Schoolcraft, BSN, RN -
Director of Crosswinds Center
Noel Jewell, M.D.,
Board Certied Psychiatry,
Board Certied Internal Medicine -
Medical Director Seneca Health
Services
Rhonda Witt, BSN, RN -
Regional Clinic Nurse
Keith DeLatte, BSW -
Care Coordinator
GREENBRIER VALLEY
MEDICAL CENTER
Connie Rose, RN -
Director Emergency Department
WEST VIRGINIA SCHOOL OF
OSTEOPATHIC MEDICINE
Raeann Carrier, Ph.D. -
Assistant Professor of Pharmacology
Victoria Shuman, D.O. -
Associate Dean of Graduate Medical
Education
FRITZ’S PHARMACY
Jennifer Ervin, PharmD -
Pharmacist
WEST VIRGINIA
PERINATAL PARTNERSHIP
Molly Scarborough McMillion RN,
BSN, IBCLC, LCCE, CTTS, CPST -
Lactation Consultant, Lamaze
Certied Childbirth Educator,
Certied Tobacco Treatment
Specialist, Special Projects
Consultant
THE GREENBRIER CLINIC
Ashlee Turner, MA -
Clinical Psychologist
STATEWIDE REVIEWERS
Mary Aldred-Crouch, MSW, MPH,
LICSW, MAC, AADC -
Manager, Substance Abuse
Treatment Services
Cabin Creek Health Systems,
Kanawha City Health Clinic
Clinical Consultant
WV DHHR, Bureau for Behavioral
Health and Health Facilities
President Elect, Public Policy Chair
WV Association of Alcoholism and
Drug Addiction Counselors
Elliott Birckhead -
Director
WV DHHR, Oce of Consumer
Aairs and Community Outreach,
Bureau for Behavioral Health and
Health Facilities
2 | Greenbrier County Care Coalition

CONTENTS
2 About Greenbrier County CARxE Coalition
THE EFFECTS OF DRUGS IN OUR COMMUNITY
4 Understanding addiction
5 Addiction is a medical condition
6 If you suspect your loved one may be abusing
7 When someone you love is addicted
8 Local stories of overcoming addiction
15 Drug Free Mother/Baby Program in Greenbrier County
16 Commonly abused prescription medications
17 Steps we can take to prevent prescription drug abuse
18 Health consequences
19 Eects during pregnancy
THE EFFECTS OF DRUGS ON OUR CHILDREN
20 Drug-exposed children: What caregivers and educators should know
22 Student concerns
23 Access to medication and medication management
24 Factors that can increase the chance of addiction
25 Why would my child use drugs?
THE EFFECTS OF DRUGS AND HOW TO HELP
26 Signs to look for
27 Things to know
28 Drugs in the workplace
29 If you suspect an overdose
30 West Virginia statutes
31 Harm reduction: the legal aspect
32 Treatment options
34 Resources
Prescription Opiate and Heroin Awareness Toolkit | 3

www.outthemonster.com
RESOURCE
It’s important to remember that
when people start taking drugs,
they don’t plan to
become addicted.
4 | Greenbrier County Care Coalition

ADDICTION IS A MEDICAL CONDITION
Addiction is a brain disease that aects a person’s priorities,
physiology and thought process.
Narcotic drugs, also known as opioids, work by binding
to opioid receptors in the brain, reducing the intensity of
pain signals that reach the brain. However, frequent use of
opioids can physically change the brain to the point where it
needs opioids to function normally. When a drug user can’t
stop taking a drug even if he or she wants to, it’s called
addiction. The urge is too strong to control, even if they
know the drug is causing harm. When people start taking
drugs, they don’t plan to become addicted. They like how
the drug makes them feel. They believe they can control
how much and how often they take the drug. However,
drugs change the brain. Drug users start to need the drug
just to feel normal. That is addiction, and it can quickly take
over a person’s life.
ADDICTION IS A BRAIN DISEASE
• Addictive drugs change how the brain works.
• These brain changes can last for a long time.
• They can cause problems like mood swings, memory
loss, even trouble thinking and making decisions.
Addiction is a disease, just as diabetes and cancer are
diseases. Addiction is not simply a weakness. People
from all backgrounds, rich or poor, can get an addiction.
Addiction can happen at any age, but it usually starts
when a person is young.
Source: www.drugabuse.gov
WHAT’S RELAPSE?
Sometimes people quit their drug use for a while, but start
using again no matter how hard they try not to. This return
to drug use is called a relapse. People recovering from
addiction often have one or more relapses along the way.
Drug addiction is a chronic (long-lasting) disease. That
means it stays with the person for a long time, sometimes
for life. It doesn’t go away like a cold. A person with an
addiction can get treatment and stop using drugs. But if he
or she started using again, they would:
• Feel a strong need to keep taking the drug
• Want to take more and more of it
• Need to get back into treatment as soon as possible
• Be just as hooked on the drug and out of control as
before
Recovery from addiction means you have to stop using
drugs AND learn new ways of thinking, feeling and dealing
with problems. Drug addiction makes it hard to function in
daily life. It aects how you act with your family, at work
and in the community. It is hard to change so many things
at once and not fall back into old habits. Recovery from
addiction is a lifelong eort.
Source: www.drugabuse.gov
Prescription Opiate and Heroin Awareness Toolkit |
5

IF YOU SUSPECT YOUR LOVED
ONE MAY BE ABUSING
While it may be necessary at some point, harsh confrontation,
accusing, and/or searching their room or personal belongings can be
disastrous. The rst step is an honest conversation.
5 TIPS FOR TALKING WITH KIDS ABOUT DRUGS AND ALCOHOL:
1 | Be open.
2 | Be non-judgmental.
3 | Treat them as individuals.
4 | Don’t make assumptions.
5 | Don’t move too fast.
SOME SUGGESTED THINGS TO TELL YOUR LOVED ONE:
I LOVE you and I’m
worried you might be
using drugs or alcohol.
I am here to
LISTEN to you.
I KNOW that drugs may
seem like the thing to do,
but doing drugs can have
serious consequences.
It makes me
FEEL worried and
concerned about you
when you do drugs.
Research shows that the
earlier a person begins to
use drugs, the more likely
they are to progress to more
serious abuse.
RESOURCE
www.Help4WV.com
38 was the average age
of the patient who visited Greenbrier
Valley Medical Center in 2015
for overdosing.
I WILL
(ll in how you
can assist)
to help you.
I WANT you to
be a part of the
solution.
6
| Greenbrier County Care Coalition

WHEN SOMEONE YOU LOVE IS ADDICTED
1 | EDUCATE YOURSELF
ABOUT ADDICTION
Search credible online
resources such as government,
university, medical and
research-based sites for the
most updated information
on addiction. Look to local
resources for information and
steps to take to stay involved.
2 | BE AWARE OF
“DOCTOR SHOPPING”
Doctor shopping is the practice
of requesting care from
multiple physicians or medical
practitioners at the same
time without coordinating
care between the practitioners
for the purpose of obtaining
narcotic prescription
medications from more than
one practitioner at the same
time.
3 | ATTEND FAMILY SUPPORT GROUPS
Alcoholics Anonymous (Al-Anon), Alateen and Narcotics
Anonymous (Nar-Anon) provide support for you and help
you nd ideas and resources from other individuals that
are facing similar challenges. Attend an Al-Anon meeting
if you cannot locate or attend a Nar-Anon meeting.
4 | SET BOUNDARIES AND LIMITS
It’s a ne line between enabling and support. Do not
provide money, access to money or other valuables.
Consider providing food and other life necessities as an
alternative. Do not accept unacceptable behavior such as
violence or abuse, drugs in your home and drugs around
children. Call local law enforcement if needed.
5 | FOCUS CONVERSATIONS TOWARD RECOVERY,
NOT BLAME
Do not threaten or shame your loved one. Reinforce that
the addiction is an illness and that you are there to assist
in the recovery process.
6 | OFFER TO ATTEND THERAPY AND BE PART OF THE
RECOVERY PROCESS
Clinicians and treatment providers cannot legally talk to
you unless your loved one asks them to and then signs a
written consent form allowing you to communicate with
the treatment provider. Ask that your loved one take care
of this.
7 | TAKE CARE OF YOURSELF!
Loving someone with an addiction can take a major toll on
your physical and mental well being. You need to take care
of yourself to continue to be the best support that you
can. Take care of basic needs such as sleep, healthy eating
and exercise. Engage in pleasurable activities regularly and
seek support for yourself.
Prescription Opiate and Heroin Awareness Toolkit | 7

THE EFFECTS OF DRUGS IN OUR COMMUNITY
LOCAL STORIES OF OVERCOMING ADDICTION
DR. PAT BROWNING’S STORY
I am Pat Browning, a retired doctor, and I have
lived in Pocahontas County for thirty-one years.
I appreciate this opportunity to talk with you
about the tragic drug epidemic that is killing
our children.
I have lost two of my three
children to this unimaginable
nightmare. I ask myself, “How
could this have happened?
Where did I fail my two
beautiful daughters?”
I’ll take you back to 1985 when my husband and
I moved to Pocahontas County with our three
adorable, brown eyed children. We moved to
a charming white house on tree lined Second
Avenue in Marlinton. Life held much promise.
My oldest child, Ariana, attended rst grade
just a few blocks away. The town was small,
but had all we needed. I truly thought, “This
is Camelot.” Then the ood of 1985 hit and
although it was devastating to our house, the
hospital, and the oce, we survived and life
was still full of hope and promise.
Ariana was seven years old
when her teacher noted she
was bright, but inattentive.
Another teacher reported
there was something dierent
about her, but couldn’t say
what it was. She had trouble
sleeping, anxiety, moodiness,
and deance. Once when she
was thirteen, a neighbor told me
she smelled marijuana coming
from our porch. She dated an
older boy, but we thought we
had it under control. To build
her self-condence we had
her work in our oce copying
various forms. Unfortunately
she was exposed to the sample medicine
closet where some nerve pills were kept. She
took several Xanax and ended up at Chestnut
Ridge Psychiatric Hospital. She was prescribed
an antidepressant, ADHD medicine, and
counseling. She was eventually homebound
schooled and then spent her senior year at a
private school in Arizona. She was diagnosed
with bipolar disorder. She often complained
her mind was racing. Looking back she may
have found drugs helped quiet those thoughts
better than her prescribed medicine.
The combination of bipolar disorder and drug
abuse is often deadly. She died of a drug
overdose at the age of twenty-three.
Much of our focus was on Ariana during that
time and our other two children were living
in turmoil and stress. Billy was busy with
school, basketball, guitar, and snowboarding.
He later told me that he was exposed to pills
in high school, but didn’t mess with them.
Izzi, however, fell into the same pattern as
Ariana. She had anxiety, trouble in school, and
exposure to drugs and alcohol. We learned
of her pain pill addiction at age twenty-two.
She went to rehab in Columbus. I moved
there for a year so she could attend out-
patient treatment and medical assistance
8 | Greenbrier County Care Coalition

school. She was placed on Suboxone to block her
cravings. I believe it saved her life for a while, but it
didn’t protect against other drugs like cocaine and
methamphetamine. She seemed to be doing well as
a medical assistant, but no matter where she went
she apparently met drug abusers and tried other
drugs. She agreed to go to rehab last summer in
Naples, Florida at the Hazelden-Betty Ford Center
where she was clean for 100 days. She was so
beautiful and serene when we visited in early October
2015. Unfortunately she “slipped up” and overdosed
on October 30, 2015 at the age of thirty-one. We
are devastated. Our daughters’ lives were so full of
turmoil, sadness, lies, and pain. Our son has lost his
two sisters, people who should be there for him when
we are gone. His 8-year-old son was inconsolable
when he heard his Aunt Izzi died.
So I stand before you today hoping my story will be
helpful to you and your children. This epidemic, like
the contagious diseases of the previous centuries does
not pick a particular type of social group. It can hit
anyone. And once drug abuse moves to addiction and
the train has left the tracks it is extremely dicult to
get it back on the tracks. Rehabilitation takes a long
time and often fails. So the key is prevention.
Evidence based research shows that there are
denite risk factors that can contribute to drug
experimentation, abuse, and ultimately addiction.
They include early aggressive behavior or dicult
temperament, ineective parental supervision and
discipline, substance abuse in the family or peers, drug
availability, and poverty. Protective factors include
good self-control, parental monitoring with clear
limits and enforcement of discipline and monitoring of
early signs of experimentation, academic competence
and success, and anti-drug use messages and policies
in the family and community.
Studies show that some children are already
abusing drugs at age 12 or 13. Early abuse often
includes tobacco, alcohol, inhalants, marijuana, and
prescription drugs such as sleeping pills, anxiety pills,
pain pills, and ADHD medicines. There is evidence that
some kids progress to addiction due to a genetic cause.
It’s like Russian roulette since we don’t know who has
the genetic vulnerability.
LOOKING BACK...
<<<
I can see many risk factors in our family.
We have a family history of alcohol abuse,
mental health issues, bipolar disorder,
depression, and suicide. I was uninformed
about the drug abuse in the community and
failed to educate my children about it. We
talked about smoking a lot since my mother
died of lung cancer. I went to medical school
when my children were going through major
transitions such as moving from elementary
school to middle school and from middle
school to high school. During these times
adolescents face many social, emotional,
and educational challenges.
Early signs of experimentation and abuse
include bloodshot eyes, change in appetite
or sleep patterns, sudden weight loss or
gain, poor grooming, unusual smells on
breath or clothing, tremors, slurred speech,
impaired coordination, and dropping grades.
From my own experience these are some of
the things I learned too late:
1. Listen to rumors about your child. They
may be true.
2. Check your child’s room frequently.
3. Perform urine drugs screens if suspicious.
4. Properly discard old medicines.
5. Lock current medicines.
6. Have clear family rules written and clear
consequences if broken. Reinforce rules at
family meetings.
7. Know your child’s peers and only allow
supervised parties with parents you trust.
8. Try to avoid major family changes. I went
to medical school at a critical time in my
children’s lives. I feel much guilt for that.
9. Have self condence in your own gut
feeling that your child may be in trouble
and immediately seek help. Children are
good liars, so trust your instincts.
Thank you for your attention. Please feel
free to ask questions now or call me if you
want. I will help you as best I can.
Dr. Pat Browning
Reference
Preventing Drug Abuse. U.S Department of
Health and Human Services National Institutes of
Health. Bethesda, MD. 2003.
Prescription Opioid and Heroin Awareness Toolkit |
9

CASEY’S STORY
I didn’t set out to get
addicted and I don’t
think anyone does.
I’m Casey. I struggle with alcohol and opioid
addiction. I have struggled with being an
addict for 18 years. Here is my long but very
real story about how I became an addict and
how I became clean.
I AM A SON
When I was 7 years old I thought I grew up in
a normal household. My dad worked all the
time and my mom stayed home and took
care of my older sister and younger brother.
My mom and grandma showed me love and
compassion. There was always a home cooked
meal and clothes on our backs.
My Dad was hardly ever around. When he and
I went hunting and shing together he would
complain about how much noise I made or
how I wouldn’t leave my line in the water long
enough. One time he hit me over the head
with a gun barrel because he was mad at me.
Looking back it’s no wonder I have so many
hang-ups now. One thing he expected of me
was to show no feelings. He would say “only
girls cry.” It is still hard for me to show feelings
to this day. He showed me a strong work ethic,
but this can be controlling too. My dad is a
workaholic. He puts work above everything
else, including family. It has been this way for
as long as I can remember. My dad is also an
alcoholic.
A BROTHER
When my brother was 4 years old he had a
stroke. He died twice and the doctors were
able to save him but he was in a coma for
seven days. On the eighth day my brother
woke up and he changed our lives forever.
When he woke up he said “I want to go
back to that pretty place.” I believe my brothe
was talking about heaven. This is when my
family started going to a church that preache
hell-re and damnation. At seven years old,
this scared me so I decided to get saved.
r
d
The leader of the church was not who he
claimed to be. He took advantage of the weak
members of the church especially the women.
He told my Mom if she would sleep with him
my brother would be healed from his seizures.
My dad ended up leaving. I blamed him for
their marriage break-up since he was never
there and always working. Then I turned my
hatred from my dad to God wondering why
God would let something like this happen.
This is when I started using alcohol at the
age of eleven. I think it was just to feel like
I belonged to a group. I was a popular kid
in school played all of the sports baseball,
football, and basketball and excelled in all
of them. At the same time my mom was
struggling and attempted suicide more times
than I can count. One time my grandma woke
me up to ambulance personnel and cops in
the house and there were messages written
in blood on the walls and refrigerator. It was
a scene straight out of a horror lm. This left
some emotional scars that I deal with today.
AN ATHLETE
Overall, my mom and I got along very well.
One of my fondest memories of my mom
was when I broke my leg she would take
me hunting and carry my gun and I would
hop along on crutches by her. She never
complained, not once. Even though we were
struggling to get through life with my broken
leg, my little brother’s seizures, and the recent
divorce with my dad, being in the woods
helped us to escape all that.
W
a
c
m
a
h
t
t
g
m
t
e started drinking together when I was
round 15 years old. I thought I had the
oolest mom in the world. I could have all of
y friends over and she would buy us alcohol
nd party with us. I thought life was grand,
aving the cool mom in town. Our addiction
o alcohol and drugs would take its toll on
his relationship. I started stealing from her t
et my x. Eventually there was no limit on
y path of my destruction. My mom would
ell me that I would steal the coins o a dead
o
A TEENAGER
10

man’s eyes if I knew it would give me my x.
We had a love-hate relationship for years.
Breaking my leg introduced me to pain pills
before anyone really knew anything about
them. Growing up I heard of alcoholics but
not addicts or junkies. Alcoholism runs on
both sides of my family but drug addiction
does not.
I always wanted acceptance from my dad and
grandpa but no matter what I was doing it was
never good enough. I have worked with my
dad a few times in the past and he was always
a lot harder on me than anyone else. I was
never good enough for dad or my grandpa. It
didn’t matter what it was, it was never up to
their standards of approval. I never really felt
loved or accepted my whole childhood and
into my adult life. This fed my addiction when
I was using drugs and alcohol. I felt accepted
and didn’t need anyone’s approval.
A STUDENT
My dad hurt me deeply inside but I showed no
feelings. I covered up my feelings with a bottle
of liquor and pain pills and it made everything
go away. I partied and drank my whole junior
high away. When I made it to high school I
was drinking a bottle of liquor every morning
before school. The teachers knew I was
drinking but said nothing. My science teacher
said once that my liver was working overtime
to heal itself, but that didn’t stop me. I still
acted like I had it all together. When I was
actually falling apart on the inside. I was trying
to ll the empty void inside of me that seemed
to keep getting bigger and bigger no matter
what I did to ll it. I hated life and wanted to
die every day. I continued this onslaught of
destruction throughout high school.
A HUSBAND
I met my wonderful wife right after high
school in the summer of 2002. We were young
and thought we had it all. I had a good paying
job and hardly any bills to pay.
I remember one of our rst dates I
asked her where she wanted to go
and she said, “to the moon.”
The following week there was a full moon and
I drove us to the tallest mountain I could nd
and said to her, “this as close as I can get.” I’m
pretty sure this was when we fell in love. We
now say, “I love you to the moon and back.”
I was enjoying every moment of life, but we
were both addicted.
Our drug addiction was getting worse by the
day. One day I received a phone call from
my grandma telling me that my mom had
attempted suicide again. I thought for sure
she was gone this time. But she survived.
About three or four days after this I got drunk
and was going to commit suicide. I loaded the
gun and shot a hole in the oor. I remember
thinking “what on earth am I doing”?
I hid the gun in one place and the clip in
another place. Eventually Krista walked out
the door leaving me alone. I decided this was
it nothing left so I went and grabbed the gun
but could not nd the clip. Krista returned
and calmed me down to nally go to sleep. I
woke up the next morning to fear and regret,
wondering if Krista was still going to leave
me. Then I realized the gun was laying there
in our room with the clip in it and I still don’t
ever remember nding it. Looking back, this
is one of the many times when God had his
hand on my life. I also have a smart, wife
who is a lot stronger than me. Both times we
found out she was pregnant she quit drugs
and alcohol cold turkey. I was selsh and used
right in front of her never giving it a thought
about what kind of struggle that I was putting
her through. I was happy about her not using
but not for the right reason though. It always
meant more drugs for me and I didn’t have
to share. I didn’t know how much hurt and
anger I brought to our relationship and those
around us.
Through all my years of addiction and chaotic
lifestyle, my wife Krista was loyal and never
left my side through the heartache and hurt
I did to her and our family. She knew deep
down inside there was a good person in there
that drugs and alcohol had covered up. Krista
was a believer in God, and I could care less
about God. I wanted to destroy God and all
Christians just like Saul in the
bible. I thought that if
God does exist he was
nothing but a big bully.
I would pray to this
God to just kill me
but it would never
happen.
T
H
E
N
Prescription Opioid and Heroin Awareness Toolkit | 11

A FATHER
We were together for ve years when our
little girl was born. When Krista was in the
hospital getting ready to have our baby. I had
to stop and buy some drugs so I wouldn’t be
sick and there was a reason to celebrate. I
just looked for any reason to get high. I was in
full addiction. When our little girl was born I
thought it would help me get sober but I just
got worse. Even then, I still didn’t think I was
that bad; at least I wasn’t sticking a needle in
my arm or out robbing someone. This went
on for a couple more years. Then we had little
boy. I was still using everyday getting worse
by the minute. I was a full-edged addict and
didn’t know any other life.
I thought, “As long as there was food on
the table and clothes on my kids’ backs,
everything was okay.” I was in denial
that my drug use wasn’t aecting them.
I kept this lifestyle for ve more years
getting worse and eventually using the
needle to get high.
My wife was still a believer and was praying
and going to church. I would insult her for
believing in God and tried to keep her and the
kids from going. I remember them getting
ready to go to church one morning and our
little girl asked “how come daddy don’t go?”
Krista told her that I was angry at God and I
would eventually get over it.
Her prayers were answered in an unusual way
on August 23, 2013. I came home in a drunken
rage. My sister called the law and Krista and
I were both lead out in handcus. We both
spent forty days in jail. The courts thought it
would scare me into getting sober but there
were just as many drugs in jail as out in the
streets. Me and some other inmates would
make jokes about the inmates who were going
to church. I was not getting any jail-house
religion. When we bonded out of jail we had t
report to the Daily Report Oce to take drug
screen tests and classes. I was still using every
day and passing the drug screens by the skin o
my teeth. I wanted to die more now than ever.
My kids were in Child Protective Services (CPS)
and I thought I would never see them again.
One day I failed a drug screen test and they
o
f
oered me rehab. They held my kids over my
head and this was my only chance of getting
them back.
This is where God intervened. The only
thing I knew about the place was I would be
there ninety days and I had to go to church
every Sunday. I told Krista I was going to tell
them I was an atheist and was not going to
church. The morning I was leaving to go I
saw Krista putting a Life Recovery Bible in my
bag. I cussed at her and threw a t like a ve
year-old kid having a temper tantrum. I was
dreading going to rehab because I wouldn’t
see my wife or my kids for ninety days and
would have no contact for 45 days. When I
arrived I told them I was an atheist and wasn’t
going to church. They told me if I didn’t go to
church I would be kicked out of rehab and I
would have no hope of getting my kids back.
When I walked into a church they took us to
NOW I HAVE
it was like walking into my worst enemy’s
A NEW
house. I felt like it would collapse on top of
PERSPECTIVE
me but it never did. The one Sunday that
changed my life was at a Baptist church and
the pastor asked us,
“If you had one day left, how would you
spend it?” I realized right there I didn’t
want to spend it high or drunk anymore.
I was still hesitant to take that step to the
alter and turn my life over to the care of God.
God whispered to me and said “If you go,
others will follow.” When I stepped out to
walk up front six guys followed me to the alter
and gave their lives to Jesus on that glorious
day. That is when God placed it on my heart
to help lead others to him who battled
addiction or whatever their hurt, habit, or
hang up might be.
It was nally time to come home from rehab
and I was ready to start this new life with God,
ready to show everyone what God had done
for me but eight days out of rehab my mom
passed away very unexpectedly. She was my
best friend. I was a momma’s boy through
and through. We were addicts together and
got sober around the same time. The last
conversation I had with her was the night
before she died and she told me she was
proud of me and she loved me.
12 | Greenbrier County Care Coalition

It is still hard not having her here with me
but I can live with the last words we spoke
to each other.
Through working the 12 principles of Celebrate
Recovery I have dealt with my demons from
the past and it helped me get over the loss
of my mom. I am now evaluating all of my
relationships. Principle six says to oer
forgiveness to those who have hurt me and
make amends for the harm I’ve done to
others, except when to do so would harm
them or others. The rst people on my
amends list were my wife Krista and kids. I
kind of knew that they would forgive me. But
when it came time to oer forgiveness to
others who hurt me it was a little bit harder.
The rst one was my sister Amanda because
she was the one that called the police and had
my children removed into the custody of CPS.
When I was in jail I thought about burning her
house down every day. But looking back, her
phone call sent the ball rolling to a changed
life. I just didn’t see it until I worked through
the principles in Celebrate Recovery. Another
person I resented was Laura the director of
Day Report in Greenbrier County. It was her
decision to send me to rehab.
Since getting right with God and others He has
opened up doors for me that I thought would
never be opened. Jeremiah 29:11, “For I know
the plans I have for you, says the Lord. They
are plans for good and not for disaster, to give
you a future and a hope.”
I have two and half years sober now. I have
my kids back and life has never been better.
I was getting caught up in doing two jobs at
one time. Working my forty an hour a week
job and doing God’s work too. I told God one
day that I can’t do both and it wasn’t a week
later and I received a message from Greenbrier
County Drug Court they were going to hire a
Peer Recovery Coach. I got the job. I still can’t
believe the plans God had for me. I lead two
Celebrate Recovery Meetings a week around
twenty guys that are dealing with Hurts,
Habits, and Hang ups.
My wife and I give Life Recovery Bibles to
anyone that is struggling. Someone gave her
one in jail and then she gave it to me and
it changed my life forever and it can do the
same for anyone if they just read it. I owe my
recovery to my wonderful wife Krista that has
stuck with me thru thick and thin and never
gave up on me when everyone else had and
to God for changing my cold heart and seeing
past all of my aws and forgiving me for
everything I did to him.
God has given me great hope for the future
when all I saw was disaster. I want to share a
Bible verse with you that really touched my
heart and that I later found out was my Mom’s
favorite verse too. It is Psalms 40:1-3, “I waited
patiently for the Lord to help me, and he
turned to me and heard my cry. He lifted me
out of the pit of despair, out the mud and miry
clay. He set my feet on a Rock and steadied me
as I walked along. He has given me a new song
to sing, a hymn of praise to our God. Many will
see what he has done and be amazed. They
will put their trust in the Lord.”
Hebrews 13:5 says, “I will never leave you nor
forsake you”. I know that is true. It can be true
for you.
Casey Butler
A rm believer in Jesus Christ
fi
NOW
Prescription Opioid and Heroin Awareness Toolkit | 13

grateful they started to
test the cord blood every
time. I walked into my
prenatal appointment not
knowing what in the world
to expect. It was my second
appointment, a lady I’d
never met before came and
got me and we sat in her
oce discussing treatment
options and all the while,
being anything but clean. One of
my options was a three-month
treatment but I did NOT want to go
down that road. I’d tried the whole
detox thing, several times. Nope,
didn’t work. I kept screening dirty
because I was as hooked as you could
get, rock bottom if you will. A couple
months went by and an extensive
treatment was pretty much my
only option (other than taking my
chances to lose my
baby, lose custody of
DAKOTA’S STORY
I am West Virginia born and bred.
It’s home sweet home but it’s also
polluted with addicts, thieves, and
drunks. I live in a small town, White
Sulphur Springs, and I’ve lived here
my whole life, other than here and
there when I was in active addiction.
Then I lived just wherever I could
aord (which isn’t much when you
have an addiction). I was pregnant
the rst time when I was 20, 21 when
my rstborn arrived into this cruel
world (girl), 23 when I had my rst
son, and 26 when I had my third
baby(boy). My addiction started after
I had my rst baby. It didn’t get too
out of hand until I was about 24ish.
Man did that take me some places
I hope to God I never return to. I
started out playing around with the
pain pills, weed, you know, the “not
so harsh crap”. When they became
harder and harder to nd, I went
to heroine, meth, whatever was
available. It wasn’t until I was 24-25
I started taking anything I could get
my hands on. Lost custody of my 2
kids because I couldn’t kick the habit.
Not for a while anyway.
When I got pregnant with my third
baby, things started to change. Back
when I had my oldest two, they
didn’t check the cord blood unless
they had a reason to, and I’m so
I took every piece of advice, took notes,
really worked hard on myself and really,
I was my own biggest critic.
I’m not going to sit here and tell
you it was all perfect because it
denitely sure wasn’t. There were
far more bad days than good, but I
took it seriously. It was either that,
or fake my way through and come
home, and waste all that time I
spent getting my head on straight.
I took every piece of advice, took
notes, really worked hard on myself
and really, I was my own biggest
critic. And man was I hard on myself.
Whoa. I’ve been clean now for
almost two years!! I can’t again, sit
here and say I’ll never go back to that
life, but I know I’m gonna bust my
butt daily to stay on the straight and
narrow. I’ve got three mini-me kids
looking up to me. I can’t disappoint
them, or myself or my family. It’s
not easy, not one bit- but is it worth
every single second? Absolutely!
him). I was absolutely
not giving them that
option to take my
baby boy after I’d
already lost custody
of two others. Nope.
So, after several
attempts and several
scary conversations
later, I nally broke
down, had to quit my job,
and go to rehab.
In 2011, 19% of babies born
at Greenbrier Valley Medical
Center had one or more
drugs in their system.
Learn more about what organizations in
Greenbrier County are doing to address the issue.
The program was great. The people
running it, the girls I was in there
with, were all a blessing. It was
normally a three-month program but
for me it was four months (I missed
a screening simply because I forgot
to look at the paper that had our
names each day to let us know who
screened that day).
At 27 years young, I’ve been through
way more than some people could
ever think about and I pray to God
every day to give me the strength to
be strong. One day at a time, take
it second by second if you have to.
I’m alive and well to write this story,
millions weren’t this lucky because
of this nasty addiction. I choose life,
you should too.
Dakota Butts
14 | Greenbrier County Care Coalition

GREENBRIER COUNTY
DRUG FREE MOTHER/
BABY PROGRAM
The Drug Free Mother/Baby
Program began when the
Greenbrier Valley Medical
Center nursery identied
that nearly 19% of
babies had been born
with one or more
drugs in their system.
During the past three
years, GVMC has seen the
number of illicit positive
newborns reduced to 6%.
For further information, call:
Tameran Asbury, MA, LSW, SAP
at 304-647-1161 or 304-646-9618.
DRUG FREE MOTHER/BABY
PROGRAM IN GREENBRIER
COUNTY
Pregnancy is a wonderful time in any woman’s
life, but can be overwhelming even in the best of
circumstances. It can be especially hard to make
good decisions under the inuence.
The Drug Free Mother/Baby Program is a
comprehensive outpatient treatment program
that works with mothers by providing prevention,
intervention, support, and treatment for women
who are pregnant or post partum. Services are
tailored to meet each mother’s individual needs.
Motivational incentives are oered to participants to
support their decision to modify their behaviors and
pursue recovery.
The primary goals of the program are to help moms
achieve their optimal goals for a healthy life and to
lessen the eects of exposure at delivery. People
make choices and we cannot take that away from
them. What we CAN do is help them make the
choices that are right for them.
RESOURCE
Prescription Opioid and Heroin Awareness Toolkit | 15

Commonly Abused Street Drugs
PERCOCET 5 MG
PERCODAN 4.5 MG
OXYCONTIN 20 MG
OXYCONTIN 80 MG
OXYCONTIN 160 MG
In 2015, Greenbrier Valley Medical
Center reported that 42% of overdose
COMMONLY ABUSED
PRESCRIPTION MEDICATIONS
PAIN MEDICATIONS
Pain medication is a class of the most abused prescription medications
among adults and teens. Opioids can be ingested in various ways.
Prescription opioids are typically taken in pill form and sometimes with
alcohol to intensify the eects. They can be crushed to sni, snort or
injected as well, such as heroin. Some commonly abused medications
include:
• Codeine (Promethazine Syrup with Codeine; Tylenol with Codeine)
• Hydrocodone (Vicodin, Lorcet, Lortab, Norco)
• Hydromorphone (Dilaudid)
• Meperidine (Demerol)
• Methadone
• Morphine (MS Contin)
• Oxycodone (Oxycontin, Roxicodone, Percocet, Endocet, Percodan)
• Buprenorphine (Suboxone/Subutex)
• Fentanyl (Sublimaze)
• Oxymorphone (Opana)
SEDATIVES
Sedatives are most commonly referred to as anti-anxiety medications
and the most abused include:
• Alprazolam (Xanax)
• Clonazepam (Klonapin)
• Lorazepam (Ativan)
• Temazepam (Restoril)
• Zolpidem (Ambien)
• Temazepam (Restoril)
• Diazepam (Valium)
STIMULANTS
Abused medications to treat ADHD/ADD include:
• Amphetamine (Adderall)
• Methylphenidate (Ritalin, Concerta)
• Steroids – are prescribed and also abused:
Anabolic steroids (Anadrol, Duraboliin, Depo-Testosterone)
visits to the ER were caused by
COMMONLY ABUSED STREET DRUGS
antidepressants or sedatives.
• Marijuana
• Methamphetamine
• Cocaine
RESOURCE
• Solvents/Aerosols
• Bath salts
• Heroin
Please visit these sites for
• LSD
detailed information about
prescription medications:
www.theantidrug.com
www.drugfree.org
www.nida.nih.gov
16 | Greenbrier County Care Coalition

STEPS WE CAN TAKE TO
PREVENT PRESCRIPTION
DRUG ABUSE
What’s in your medicine cabinet?
On your nightstand?
On the kitchen counter?
In your purse?
Naturally, you keep prescription medicines and
cold and cough remedies handy for you to take
when needed. They are also handy for everyone
else to take without you knowing it.
1 | LOCK YOUR MEDS
Only 4.7% of individuals who abuse
prescription drugs, say they get the
medication from a stranger, drug dealer,
or the Internet. Prevent your children from
abusing your medications by securing them
in places they cannot access. Lock them up or
take them out of your house.
www.walmart.com/ip/
sentrysafeelectronic- security-box
2 | TAKE INVENTORY
Use a home medication inventory card to
record the name and amount of medications
you currently have. Check regularly to make
sure none are missing. For a printable home
medication inventory card, visit
www.trumbullmhrb.org/pdfs/
Inventory-Card.pdf
3 | EDUCATE YOURSELF AND YOUR CHILD
Learn about the most commonly abused
types of medications (pain relievers,
sedatives, stimulants and tranquilizers). Then
communicate the dangers of abusing these
medications to your child regularly –
ONCE IS NOT ENOUGH!
The U.S. makes up only 4.6%
of the world’s population
but consumes 80% of its
opioids and 99% of the
world’s hydrocodone, the
opioid that is in Vicodin.
ABC News and the National Drug
Court Institute Fact Sheet Volume
XI, No.2.
In West Virginia in
2015, there were 643
overdose deaths.
4 | SET CLEAR RULES AND
MONITOR BEHAVIOR
Do not allow your child to take prescription
drugs without a prescription. Monitor your
child’s behaviors to ensure that rules are
being followed. Lead by example!
5 | PASS IT ON
Share your knowledge, experiences and
support with the parents of your child’s
friends. Work together to ensure that your
children are safe and healthy.
6 | DISPOSE OF OLD AND
UNUSED MEDICATIONS
These public drop boxes are visible and
always open.
GREENBRIER COUNTY COURTHOUSE
912 Court St. N.
Lewisburg, WV 24901
(304) 647-6694
RUPERT SHERIFF’S OFFICE
530 Nicholas St.
Rupert, WV 25984
(304) 392-6320
More than 6.2 million people age 12
and older report abusing prescription drugs.
Many teens believe prescription drugs are a safe way to get high
due to the fact that they improve health when used as prescribed.
It is illegal to use someone else’s prescription.
17

HEALTH CONSEQUENCES
Prescription medication abuse and intravenous drug
use has an adverse eect on your health.
Drugs alter
a person’s thinking and
judgment
Drug use and abuse weakens the immune system.
Learn more at www.drugabuse.gov.
abuse, including the illegal use of prescription medication, is associated
The potential for physical and psychological addiction is real. Drug use and
RESOURCE
with strong cravings for the drug, making it dicult to stop using. Most
drugs alter a person’s thinking and judgment, which can increase the risk
of injury or death from drugged driving or infectious diseases.
ALTERED JUDGMENT AND THINKING DUE TO
PRESCRIPTION MEDICATION ABUSE CAN LEAD TO:
• Depression
• Seizures
• Hallucination
• Unsafe sex or needle sharing,
which can lead to...
►
HIV/AIDS
►
Hepatitis B and C
►
Chlamydia
►
Gonorrhea
►
High risk HPV
►
Genital warts
►
Herpes and Syphilis
►
Unintended pregnancy/NAS (Neonatal Abstinence
Syndrome) is a condition in which a baby can suer from
dependence and withdrawal symptoms after birth.
PREVENT HEPATITIS C AND HIV
The use of unclean needles and injection
equipment is dangerous. Sharing needles,
syringes, and other injection equipment
is a direct route of HIV and/or Hepatitis
C transmission. HIV stands for human
immunodeciency virus. If untreated, the virus
that can lead to acquired immunodeciency
syndrome (AIDS). Unlike some other
viruses, the human body can’t get rid of HIV
completely, even with treatment. So once you
get HIV, you have it for life. Hepatitis C is a
serious liver disease caused by a virus that can
range in severity from a mild illness lasting
a few weeks to a serious, lifelong illness.
The risk for getting HIV or Hepatitis C is high
if a person uses injection equipment that
someone with HIV or Hepatitis C has used.
This high risk is because the drug materials
may have blood in them, and blood can carry
HIV and/or Hepatitis C. Bleaching, boiling,
burning, or using common cleaning uids,
alcohol, or peroxide will not kill the Hepatitis
C virus. The Hepatitis C virus is dicult to kill.
So although cleaning equipment may reduce
the amount of virus, it does not eliminate it.
Sources: CDC 2016 (https://www.cdc.gov/hiv/
pdf/risk/cdc-hiv-idu-fact-sheet.pdf) and CDC 2015
(https://www.cdc.gov/hepatitis/HCV/PDFs/
FactSheet-PWID.pdf)
18 | Greenbrier County Care Coalition

EFFECTS DURING
PREGNANCY
Neonatal Abstinence Syndrome (newborn withdrawal)
is a group of signs and symptoms that a baby can
have when a mother takes certain medications or
other drugs during her pregnancy. These substances
may include methadone, subutex/suboxone, heroin
and other prescription medications such as Oxycontin
and Vicodin. Babies exposed to these drugs any time
in pregnancy have an 80% chance of developing
withdrawal symptoms.
SYMPTOMS OF WITHDRAWAL INCLUDE:
• High-pitched crying or dicult to console
• Poor feeding, spitting up, vomiting, diarrhea
• Diculty sleeping
• Overly vigorous suck or uncoordinated suck
• Tremors, jitteriness
• Occasionally seizures can occur
• Frequent hiccups and/or sneezing
• Mild fever
• Sweating
Infants with known exposure to drugs during pregnancy
are observed in the hospital for a minimum of 72 hours
after birth. A segment of the infant’s umbilical cord
is sent away for testing at birth. During that time,
symptoms are monitored for severity by sta and
“scored” every four hours using a tool like the Modied
Finnegan Neonatal Abstinence Score sheet.
Caregivers and parents are taught to use “Therapeutic
Handling” techniques to help keep scores down, and the
environment is kept as minimally stimulating as possible.
Infants with consistently high schores are usually started
on medication to control their symptoms and prevent
seizures. Medications like methadone, morphine and
phenobarbital are carefully prescribed and administered
to control symptoms. The exact length of time it takes
to wean these substances diers from baby to baby. It is
not unusual for babies to be in the hospital for 2-6 weeks.
Once they are weaned from medication and scores are
consistently low, the baby will be discharged from the
hospital.
Per federal law, umbilical cord tissue results that are
positive for drugs – whether prescribed or not – must
be reported to Child Protective Services, who will
then make a determination of safety for the infant. It
is particularly important that infants who are stable
for discharge – whether they have been treated
for withdrawal or not – must still be kept in low
stimulation environments, with gradual introduction
of stimuli so as to avoid relapse at home. Consistent
visits to the pediatrician, along with developmental
follow up (such as Birth to Three), is essential.
For more information about
RESOURCE
Neonatal Abstinence Syndrome
or eorts in the state of West Virginia, go to
www.wvperinatal.org, the website of the
WV Perinatal Partnership or contact:
Molly Scarborough McMillion
(304) 667 - 4362
mmcmillion@osteo.wvsom.edu
Prescription Opioid and Heroin Awareness Toolkit | 19
?
?
THE EFFECTS OF DRUGS ON OUR CHILDREN
Behaviors
you see might be the
only way children can
express their
feelings
DRUG-EXPOSED CHILDREN:
WHAT CAREGIVERS AND
EDUCATORS SHOULD KNOW
EMOTIONAL
• Seems sad or does not enjoy activities
• Takes on a lot of guilt and blames
themselves for what goes wrong
• Feels their life will always be bad
• May attach to strangers too easily, but
have diculty trusting caregivers
COGNITIVE
• Diculty talking and listening
• Diculty remembering a list of things
• Diculty remembering what they were
just told
• Often do not learn from mistakes
or experiences
What is a drug exposed child?
A drug exposed child can be identied as any
child whose brain and/or body has been aected
because his/her parents used drugs or alcohol
during pregnancy, and/or who is living in a home
where drugs are abused and/or illegally made,
traded or given away.
BEHAVIORAL
• Likes to be alone
• Finds change dicult
• Doesn’t get along well with other
people
• Doesn’t seem to care about what
happens to them
• More interested in sex and drugs or
may know more about sex and drug-
related topics than most children
their age
• Tells detailed stories involving drug
use, drug deals or other indications
of illegal activity, such as suspicious
adult behavior. (Mom sometimes
takes medicine and sleeps all day)
• Has a strong distrust of authority
gures and the police
Remember, not every behavior indicates a specic concern.
20 | Greenbrier County Care Coalition

Children are dying from
abuse and neglect at a
higher rate in West
Virginia than in any
other state.
In West Virginia, 16 children died
in 2016 from abuse and neglect
at a rate of 4.16 children per 100,000.
Source: National Child Abuse and Neglect Data Systems.
HELPING A DRUG ENDANGERED CHILD
Prenatal drug exposure can cause damage to
the developing brain. What you think is “odd”
or dicult behavior might be something the
child cannot control. Try to understand that the
“behaviors” you see might be the only way that a
child can express his/her feelings. You can help by:
• Be repetitive. Do things the same way, every
time, over and over again.
• Keep things quiet and calm.
• Be realistic about what you expect, and
understand that drug-exposed children may
not act their age.
• Give support and encouragement.
• Help them feel safe.
• Help them separate the parent from the
substance abuse.
• Allow them periods of grief.
• Teach them empathy by showing
understanding, sympathy and compassion.
Show them you care by being
understanding, sympathetic
and compassionate.
21

22 | Greenbrier County Care Coalition
Results indicated that nearly
one in three students
(29.2%) who participated
in the survey had used
prescription drugs in the
past 30 days.
Two hundred and twenty-
three students in Greenbrier
County high schools and
middle schools were surveyed
about prescription drug
use during the fall of 2016.
Students ranged in age
from 11-19. Respondents
were fairly evenly split in
terms of gender with 47% of
respondents being male and
50% being female (3% did not
disclose their gender).
Students who abuse
prescription stimulants
(e.g. ADHD medication
Adderall and Ritalin)
reported higher levels of:
cigarette smoking, heavy
drinking, risky driving,
abuse of marijuana, abuse
of MDMA (Ecstasy) and
abuse of cocaine.
Source: Harvard School of Public
Health, College Health Study,
2001 Survey
WHERE ARE
PRESCRIPTION DRUGS
OBTAINED BY TEENS?
6%
Taken from a friend
22%
Free from a friend
6%
Bought from
a friend
33%
Bought from a drug
87%
dealer or stranger
3%
Bought on
the internet
4%
Prescribed by more
than one doctor
26%
Prescribed by
one doctor
Where?
STUDENT CONCERNS
In September 2016 the West Virginia State Board of Education approved a new
policy that will allow schools across the state to stock intranasal naloxone
or Narcan to help deal with overdoses. School boards can now enact policy
changes that will allow them to carry the drugs in their schools. As part of
the new policy only school nurses with a RN or LPN license can administer the
life-saving drug that reverses the eect of opioids in an overdose situation.
Greenbrier County Schools Board of Education is creating policy to be in line
with the West Virginia Department of Education.
TOP REASONS GREENBRIER COUNTY
TEENS USE PRESCRIPTION DRUGS
It was prescribed
to me by my
physician

According to the Center for
Disease Control (CDC),
enough painkillers
will be prescribed this
year to medicate every
American adult around
the clock for a month.
ACCESS TO MEDICATION AND
MEDICATION MANAGEMENT
What are your kids being prescribed?
Think before you ll and give a pain prescription to your child.
Do they really need such a strong medication or will something
else do? Pain medications, like Vicodin, Oxycontin, and other
versions are strong. We live in a high prescribing region of the
state. Youth are not an exception. They are being prescribed
large quantities of strong medications for things such as simple
sports injuries and dental procedures. Be an advocate while you
can and look into all options. Pain is no fun, but it’s better than
starting an addiction in your child.
vs.
West Virginia led the nation in
prescriptions lled or relled per capita in
2008. The national average of number of
prescriptions per patient is 12.
The West Virginia average of number
of prescriptions per person is 18.7.
Source: Kaiser Family Foundation, State Health
Facts at www.statehealthfacts.org
24 hours
for 1 month
BE PROACTIVE WHEN IT COMES
TO YOUR CHILD’S MEDICATION
Consider asking the physician or a
pharmacist the following questions
before lling a prescription:
• What are some alternatives for
pain management?
• Can you prescribe a non-opioid
pain medication?
• If my child must take opioids for
pain relief, how can I minimize
risks of dependency?
• If you must prescribe an opioid,
limit the quantities.
MEDICATION DISPOSAL INFORMATION
These public drop boxes are visible and always open.
GREENBRIER COUNTY
RUPERT SHERIFF’S OFFICE
COURTHOUSE
530 Nicholas St.
912 Court St. N.
Rupert, WV 25984
Lewisburg, WV 24901
304.392.6320
304.647.6694
PROPERLY DISPOSING UNUSED
MEDICATION CAN DECREASE THE
CHANCE OF A CHILD GAINING
ACCESS TO MEDICATION.
www.Help4WV.com
The Help4WV hotline received
61 calls from Greenbrier
County residents alone
during an approximate 17 month
time period.
Source: Help4WV summary report
Sept. 9, 2015 through Dec. 18, 2016.
Prescription Opioid and Heroin Awareness Toolkit |
23

FACTORS THAT CAN INCREASE THE
CHANCE OF ADDICTION
40-60%
of a person’s vulnerability to
addiction stems from
genetic factors.
As with any other disease, the capacity
to become addicted diers from person
to person. In general, the more risk
factors a person has, the greater the
chance that taking drugs will lead to
abuse and addiction.
(Excerpted from Drugs, Brains, and Behavior:
The Science of Addiction by NIDA)
archives.drugabuse.gov/NIDA_Notes/
NN05index.html
RESOURCE
24 | Greenbrier County Care Coalition
1 | HOME AND FAMILY
• Inuence during childhood is an
important factor
• Parents or older family members
who abuse drugs or engage in
criminal behavior can increase
children’s risks of developing
their own drug problems
2 | PEERS AND SCHOOL
• Drug-using peers can sway even
those without risk factors to try
drugs
• Academic failure
• Poor social skills can put
a child at further risk for
using drugs
3 | BIOLOGICAL FACTORS
• Genetic factors account
for 40-60% of a person’s
vulnerability to addiction
• Environmental factors aect
the function and expression
of a person’s genes
• A person’s stage of
development and other
medical conditions
• Adolescents and people with
mental disorders are
at greater risk of drug
abuse and addiction than the
general population
4 | METHOD OF
ADMINISTRATION
• Smoking a drug or injecting
it into a vein increases its
addictive potential
• Both smoked and injected
drugs enter the brain
within seconds
• This intense “high” can fade
within a few minutes, taking
the abuser down to lower,
more normal levels
5 | EARLY USE
• Research shows that the
earlier a person begins to
use drugs, the more likely he
or she is to develop serious
problems
• This reects the harmful
eect that drugs can have on
the developing brain
• It is a strong indicator of
problems ahead, including
addiction

Know that you will have
this discussion many times.
Talking to your child
about drugs and alcohol
is not a one-time event.
WHY WOULD MY CHILD USE DRUGS?
In general, people begin taking drugs for a variety of reasons.
TO FEEL GOOD
Most abused drugs produce intense feelings of pleasure.
This initial sensation of euphoria is followed by other
eects, which dier with the type of drug used. For
example, with stimulants such as cocaine, the “high”
is followed by feelings of power, self-condence and
increased energy. In contrast, the euphoria caused
by opioids such as heroin, is followed by feelings of
relaxation and satisfaction.
TO FEEL BETTER
Some people who suer from social anxiety, stress-
related disorders and depression begin abusing
drugs in an attempt to lessen feelings of distress.
Stress can play a major role in beginning drug use,
continuing drug abuse or relapse in patients recovering
from addiction. To do better, some people feel pressure
to chemically enhance or improve their cognitive or
athletic performance, which can play a role in initial
experimentation and continued abuse of drugs such as
prescription stimulants or anabolic/androgenic steroids.
CURIOSITY AND “BECAUSE OTHERS ARE DOING IT”
In this respect, adolescents are particularly vulnerable
because of the strong inuence of peer pressure. Teens
are more likely than adults to engage in risky or daring
behaviors to impress their friends and express their
independence from parental and social rules.
(Excerpted from Drugs, Brains, and Behavior: The Science of
Addiction by NIDA)
If
drug test, contact your local pharmacy.
you are interested in obtaining a home
RESOURCE
25
THE EFFECTS OF DRUGS AND HOW TO HELP
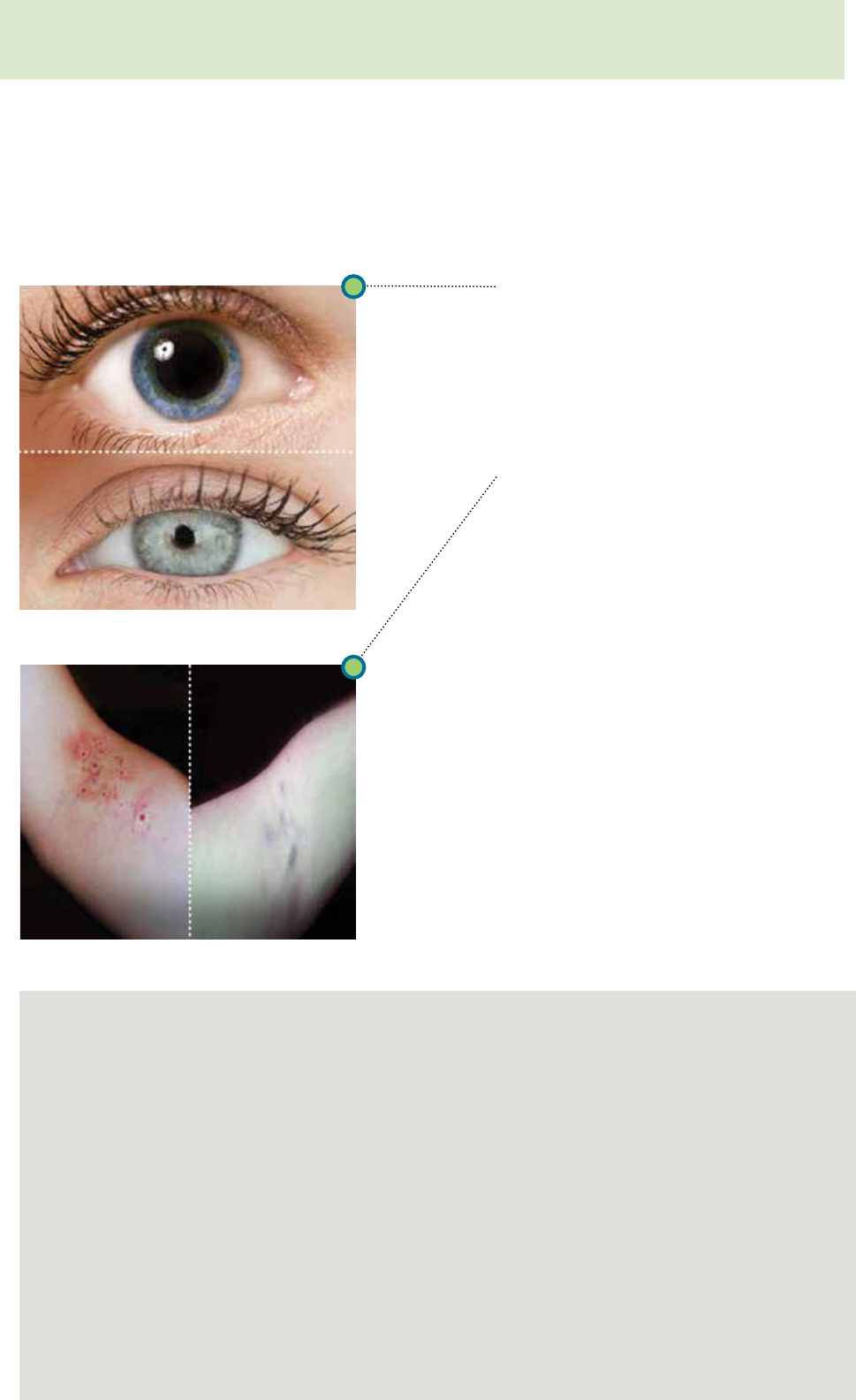
SIGNS TO LOOK FOR
The duration of a dose of heroin can last three to six hours and be detected up to two
days. Physical and behavioral signs and symptoms of opioid intoxication include:
DILATED PUPILS
CONSTRICTED PUPILS
FRESH TRACK MARKS TRACK MARKS MORE
THAN 10 DAYS OLD
PHYSICAL
• Constricted/pinpoint pupils
• Sweating
• Lower body temperature
• Flushed skin
• Decreased heart rate
• Decreased blood pressure
• Asthma attacks in asthmatic
individuals that inhale the drug
• Depressed breathing
• Track marks
COGNITIVE
• Clouded mental function
• Impaired coordination
• Slurred speech
• Slowed reexes
BEHAVIORAL
• Euphoria or euphoria followed
by drowsiness
• Decreased appetite
• Dry mouth/thirsty
• Itching/scratching
• Suppressed pain
• Mood swings
• Apathy
• Depression
• Feeling of heavy limbs
THE OVERLAP BETWEEN OPIOID ADDICTION AND BEHAVIOR
Opioid addiction is a distressing problem that
often includes mental health concerns. The
overlapping issues of non-medical opioid use
and mental health make identication of
these co-morbid problems both complex and
necessary for appropriate clinical care. Cognitive
and behavioral symptoms that may occur with
opioid use include confusion, poor judgment,
depression, anxiety, paranoia, hallucinations,
delusions, anger, and suicidal ideations.
Source: Opioid Use Behaviors, Mental Health and Pain
Development of a Typology of Chronic Pain Patients.
National Institute of Health. Drug Alcohol Depend.
2009, September 1; 104 (1-2): 34-42).
LIFESTYLE CHANGES THAT CAN BE
RELATED TO OPIOID ADDICTION
• A change in peer group
• Missing classes, skipping school or work
• Loss of interest in favorite activities
• Trouble in school or with the law
• Changes in appetite or sleep patterns
• Losing touch with family members and friends
• Money loss, asking for monetary loans or
missing items from family/friends
26

THINGS TO KNOW
“
SLANG
• Snorted, injected, swallowed and inhaled
• Crushed pills are snorted and inhaled using short
straws, rolled dollar bills and other small tubing
• Mirrors, razor blades or credit cards might be used in
preparing the drug
• Syringes, rubber tubes, syringe caps, droppers and
spoons are used when preparing or injecting the drug
• To inhale the drug, pipes or pieces of rectangular
aluminum foil (3x17cm) are used
• Empty packaging such as corner ties and tin foil squares
HEROIN:
Black
Black Eagle
Black Pearl
Black Stu
Boy
Brown
Brown Crystal
Brown Rhine
Brown Sugar
Brown Tape
Chiba
China
China White
Chiva
Dope
Dragon
H
Junk
Mexican Brown
Mexican Horse
Mexican Mud
Number 3
Number 4
Number 8
Sack
Scat
Skag
Smack
Snow
Snowball
White
White Boy
White Girl
White Horse
White Lady
White Nurse
White Stu
USING HEROIN:
Channel swimmer
Chasing the Dragon
Daytime (being high)
Dip and Dab
Do up
Evening (Coming o the high)
Firing the Ack Ack Gun
Give Wings
Jolly Pop
Paper Boy
OXYCONTIN, PERCOCET, VICODIN
AND OTHER PAINKILLERS:
Big Boys
Cotton
Kicker
Morph
Tuss
Vike
Watson-387
USING PRESCRIPTION DRUGS
AND ABUSE:
Pharming
Pharm Parties
Recipe (mixing with alcohol)
Trail Mix
USING HEROIN + OTHER DRUGS:
Heroin + Alprazolam (Xanax): Bars
Heroin + Cocaine:
Belushi
Boy-Girl
He-She
Dynamite
Gooall
H&C
Primo
Snowball
Heroin + Cold Medicine: Cheese
Heroin + Crack:
Chocolate Rock
Dragon Rock
Moonrock
Heroin + Ecstasy:
Chocolate Chip Cookies
H Bomb
Heroin + LSD:
Beast
LBJ
Heroin + Marijuana (THC):
Atom Bomb
Canade
Woola
Wookie
Woo-Woo
www.caspalmera.com/nicknames-
stree-names-and-slang-for-heroin/
RESOURCE
“
Prescription Opioid and Heroin Awareness Toolkit | 27

DRUGS IN THE WORKPLACE
Industries that tend to
have a higher number of
substance users include:
Construction
Trucking
Retail sales clerks
Assembly and
An es
10-
timated
12%
of employees use
alcohol or illegal drugs
while at work.
manufacturing workers
(SAMHSA) This number doesn’t
include people who abuse opioid
drugs, under a physician’s
prescription, at work.
70%
of substance
abusers hold jobs,
according to the American
Council for Drug Education
(ACDE)
Drug abuse costs employers
$81 billion annually
according to estimates by the National
Council on Alcoholism and Drug
Dependence, Inc.
in
3.6x more likely to be
volved in on-the-job accidents
Responsible for
40%
of all industrial fatalities
The following statistics provided
by ACDE show how drug abuse
aects employees and employers
because using employees are:
10x more likely to miss work
w
5x more likely to le a
orker’s compensation claim
33% less productive
Responsible for
health care costs nearly 3x
that of their non-using peers
JOB PERFORMANCE AND
WORKPLACE BEHAVIORS
MAY BE SIGNS THAT
INDICATE POSSIBLE WORK
PLACE DRUG PROBLEMS:
JOB PERFORMANCE
• Inconsistent work quality
• Poor concentration and lack
of focus
• Lowered productivity or
erratic work patterns
• Increased absenteeism or on
the job “presenteeism”
• Unexplained disappearances
from the job site
• Carelessness, mistakes, or
errors in judgment
• Needless risk taking
• Disregard for safety of self
and others on the job and o
the job accidents
• Extended lunch periods and
early departures
WORKPLACE BEHAVIOR
• Frequent nancial problems
• Avoidance of friends and
colleagues
• Blaming others for own
problems and shortcomings
• Complaints about problems
at home
• Deterioration in personal
appearance or personal
hygiene
• Complaints, excuses and
time o for vaguely dened
illnesses or family problems
28 | Greenbrier County Care Coalition

IF YOU SUSPECT
AN OVERDOSE
Dos and don’ts in responding
to opioid overdose
An opioid overdose requires immediate
medical attention. An essential rst step
is to get help from someone with medical
expertise as soon as possible.
CALL FOR HELP. DIAL 911 TO
ACTIVATE EMERGENCY SERVICES.
AN OPIOID OVERDOSE NEEDS
IMMEDIATE MEDICAL ATTENTION.
1 | All you have to say is: “Someone is
not breathing.”
2 | Be sure to give a clear address and/or
description of your location.
DO support the person’s breathing by
administering oxygen or performing rescue
breathing.
DO administer naloxone (NARCAN).
GVMC ER
OVERDOSE
VISITS IN 2015
DO stay with the person and keep
him/her warm.
DON’T slap or try to forcefully stimulate
the person — it will only cause further
injury. If you are unable to wake the person
by shouting, rubbing your knuckles on the
sternum, or light pinching, he or she may be
unconscious.
DON’T put the person in a cold bath or
shower. This increases the risk of falling,
drowning or going into shock.
DON’T inject the person with any
substance (salt water, milk, “speed,” heroin,
etc). The only safe and appropriate treatment
is naloxone.
DON’T try to make the person vomit
drugs that he or she may have swallowed.
Choking or inhaling vomit into the lungs can
cause a fatal injury.
www.samhsa.org
RESOURCE
In 2015, Greenbrier Valley Medical Center reported
52% of overdose visits in the ER were a result of
opioids and heroin abuse
and 71% of all overdoses
in the ER were female.
52%
RESULTED
FROM OPIOIDS
AND HEROIN
ABUSE
71%
OF ALL
OVERDOSES
ERE FEMALE W
HAVE NARCAN ON HAND
If you administer Narcan, calling 911 will enact the “Good Samaritan” law.
Narcan can be given by intramuscular injection into the muscle of the arm, thigh
or buttocks or with a nasal spray device (into the nose). Don’t wait for help if
you are with someone who is overdosing. With basic training, friends and family
members can recognize when an overdose is occurring and give Narcan.
SIGNS OF AN OVERDOSE,
which is a life-threatening
emergency, include:
SIGNS OF OVER MEDICATION,
which may progress to overdose,
include:
• Face is extremely pale and/or
clammy to the touch
• Body is limp
• Fingernails or lips have a blue or
purple cast
• The individual is vomiting or
making gurgling noises
• He/she cannot be awakened from
sleep or is unable to speak
• Breathing is very slow or stopped
• Heartbeat is very slow or stopped
• Unusual sleepiness or drowsiness
• Mental confusion, slurred speech,
intoxicated behavior
• Slow or shallow breathing
• Pinpoint pupils
• Slow heartbeat, low blood pressure
• Dicult waking the person
from sleep
Prescription Opioid and Heroin Awareness Toolkit | 29

WEST VIRGINIA STATUTES
As of May 26, 2017
DIRECTLY DRUG RELATED
INDICTMENTS IN GREENBRIER CO.
69%
56%
45%
43%
41%
>
25%
JUNE OCT. FEB. JUNE OCT. FEB.
2014 2014 2015 2015 2015 2016
Since 2013, the Greenbrier Valley
Drug and Violent Crime Task
Force has indicted an additional 26
individuals in U.S. Federal Court
involving opioid and heroin cases.
**
MORE THAN /
45 DRUG RELATED
INDICTMENTS
FEB.
2014
WERE METH RELATED
MANUFACTURE,
DISTRIBUTION OR MANUFACTURE, DISTRIBUTION
DR
UG NAME
POSSESSION
STATUTE
POSSESSION PENALTIES*
POSSESSION WITH INTENT
TO DELIVER STATUTE
OR POSSESSION WITH INTENT TO
DELIVER PENALTIES
MARIJUANA
§60-4-401(c)
90 days to 6 months
and/or a ne of up to $1,000
§60-4-401(ii)
1-5 years in prison and/or
up to a $15,000 ne
2nd and subsequent
up to a year in jail and/or up to a
$2,000 ne
2-10 years in prison and/or
up to a $30,000 ne
(1-15 years depending on the schedule)
PRESCRIPTION
NARCOTIC DRUG
§60-4-401(c)
90 days to 6 months
and/or a ne of up to $1,000
§60-4-401(ii)
1-5 years in prison and/or
up to a $15,000 ne
2nd and subsequent
up to a year in jail and/or up to a
$2,000 ne
2-10 years in prison and/or
up to a $30,000 ne
HEROIN
§60-4-401(c)
90 days to 6 months
and/or a ne of up to $1,000
§60-4-401(i)
1-5 years in prison and/or
up to a $25,000 ne
2nd and subsequent
up to a year in jail and/or up to a
$2,000 ne
2-30 years in prison and/or up to a
$50,000 ne
COCAINE
§60-4-401(c)
90 days to 6 months
and/or a ne of up to $1,000
§60-4-401(i)
1-5 years in prison and/or
up to a $25,000 ne
2nd and subsequent
up to a year in jail and/or up to a
$2,000 ne
2-30 years in prison and/or up to a
$50,000 ne
METHAMPHETAMINE
§60-4-401(c)
90 days to 6 months
and/or a ne of up to $1,000
§60-4-401(ii)
1-5 years in prison and/or
up to a $15,000 ne
2nd and subsequent
up to a year in jail and/or up to a
2-10 years in prison and/or
up to a $30,000 ne
$2,000 ne
FENTANYL
§60A-4-414(b)
(1) Less than one gram, 2-10 years
in prison
§60A-4-414(b)
(1) Less than one gram, 2-10 years
in prison
(2) One gram or more but less
than ve grams, 3-15 years
in prison
(3) Five grams or more, 4-20 years
in prison
(2) One gram or more but less
than ve grams, 3-15 years in prison
(3) Five grams or more, 4-20 years
in prison
* Note: Conditional discharge is available for rst offense of possession by ordering the accused to a period
of probation before trial. The court proceedings are deferred during this period. If probation is successfully
completed, the charges may be dismissed.
30 | Greenbrier County Care Coalition
**Source: Greenbrier County Probation Ofce

THANK YOU,
HARM REDUCTION:
THE LEGAL ASPECT
Elliott Birckhead, Director
Ofce of Consumer Affairs and
Community Outreach, Bureau
for Behavioral Health and
Harm reduction is a set of practical strategies
and ideas aimed at reducing negative
consequences associated with drug use.
As of May 26, 2017
JUSTICE REINVESTMENT BILL
Senate Bill 371, the West Virginia Justice Re-Investment
Act, was signed into law during the 2013 regular
legislative session. The bill implements policy changes
developed through “justice reinvestment,” a data-
driven approach designed to improve public safety,
reduce corrections spending, and reinvest savings
in strategies that can decrease crime and reduce
recidivism. One branch of the bill focused on the issue
of substance abuse via investment in community-
based treatment for people on supervision with
substance use treatment needs; establishment of
partnerships and resources across systems; and
ensuring eective substance abuse treatment within
state prisons.
Senate Bill 335, the Creating Access to Opioid
Antagonists Act, was signed into law during the
2015 regular session. This bill allows licensed health
care providers to prescribe opioid antidote to initial
responders and to a person considered by the licensed
health care provider to be at risk of experiencing
an opioid-related overdose, or to a relative, friend,
caregiver or person in a position to assist a person at
risk of experiencing an opioid-related overdose. The bill
also provides for limited liability for initial responders,
licensed health care providers who prescribe opioid
antagonist in accordance with this article, and for
anyone who possesses and administers an opioid
antidote.
Senate Bill 431, authorizing pharmacists and pharmacy
interns to dispense Naloxone, was signed into law
during the 2016 regular session. This bill authorizes
pharmacists or pharmacy interns to dispense,
pursuant to a protocol, Naloxone without
a prescription.
CALL 911 WITHOUT RISK
Senate Bill 523, the Creating Alcohol and Drug
Overdose Prevention and Clemency Act, was signed
into law during the 2015 regular session. The bill
provides immunity from prosecution in limited
circumstances for persons who call for emergency
medical assistance on behalf of people who reasonably
appear to be experiencing a drug or alcohol overdose.
Health Facilities,
FOR YOUR ADVISEMENT
AND CONTRIBUTIONS.
HERE IS A SOURCE FOR LEARNING MORE
ABOUT ANY GIVEN BILL. LINK TO THE BILL
STATUS PAGE ON THE LEGISLATIVE WEBSITE:
www.legis.state.wv.us/Bill_Status/bill_status.cfm
Enter the bill number and it will pull the bill history
and includes links to the nal version of the bill, also
called the enrolled bill.
HOUSE BILL 2195 - Requires comprehensive drug
awareness and prevention program in all public
schools and requires county boards to implement no
later than 2018-2019 school year.
SENATE BILL 386 - The West Virginia Medical
Cannabis Act; Details the eorts to establish a medical
cannabis program; placing the medical cannabis
program within the Department of Health and Human
Resources and under the direction of the Bureau for
Public Health; establishing lawful use and forms of
medical cannabis.
HOUSE BILL 2329 - Prohibits the production,
manufacture or possession of fentanyl.
HOUSE BILL 2579 - Relates to the oense
of transporting illegal substances into the
state generally; increasing penalties for illegal
transportation of controlled substances into the state.
HOUSE BILL 2585 - Relates to laundering of proceeds
from specied criminal activities generally.
SENATE BILL 220 - Creates a felony oense of
delivering controlled substances or counterfeit
controlled substances for an illicit purpose resulting
in the death of another person and provides criminal
penalties accordingly.
SENATE BILL 76 - Creating WV Second Chance for
Employment Act. Allows people who have completed
serving felony oenses for drug crimes to le to
have their felonies reduced to misdemeanors. This
bill relates to establishment of a criminal oense
reduction program. It creates the criminal oense
classication of reduced misdemeanor, which allows
persons convicted of certain criminal felony oenses
to petition under specied circumstances for reduction
of the felony to misdemeanor status.
Prescription Opioid and Heroin Awareness Toolkit | 31

TREATMENT OPTIONS
DETOX OR DETOXIFICATION IS THE FIRST STEP
TOWARD RECOVERY
This is when an individual will stop using heroin and begin
to overcome physical dependence on the drug. Often
individuals will return to use to stop the pain and adverse
eects of the heroin withdrawal. The eects of withdrawal
will vary from person to person depending on various
factors including the frequency and dose of use as well as
the length of time using. Individuals can seek assistance
with the withdrawal from a local emergency room, a
primary care physician or on a behavioral health unit.
INPATIENT
Inpatient refers to a behavioral health unit or a psychiatric
hospital with a length of stay from a couple of days to a
couple of weeks. Inpatient care involves that detox process,
as well as limited individual and group therapy.
RESIDENTIAL TREATMENT
Residential treatment is a 28 -90 day program in which
an individual resides in a facility specic to substance
abuse treatment. Individuals are immersed in treatment
throughout their day.
PARTIAL HOSPITALIZATION AND DAY TREATMENT
Partial hospitalization and day treatment involve attending
a treatment facility daily while staying home at night.
INTENSIVE OUTPATIENT
Intensive outpatient is a group therapy that is conducted
two to four times per week for more than an hour at a time.
Outpatient counseling and therapy is individual counseling
that is conducted one to two hours per week to address
any previous trauma or pain that may have led to and been
a result of their drug use. Counseling can also help identify
any triggers and assist in preventing relapse.
Transitional living or half-way houses are sober group living
environments. There are no substance abuse treatments
in the home. Rather, it is a group of individuals living in a
structured environment in eorts to maintain sobriety.
SUPPORT GROUPS
Groups such as a 12-step Narcotics Anonymous and
Celebrate Recovery are usually peer-driven meetings to
oer social supports and connections.
32
| Greenbrier County Care Coalition

Medication-assisted treatment (MAT) uses behavioral health
treatment combined with medications such as buprenorphine,
naltrexone, or methadone to manage the withdrawal
symptoms and cravings for heroin, other opioids, or alcohol
while fostering recovery from the brain disease of addiction.
This type of treatment is typically done in an outpatient setting.
Physicians are required to undergo specic addiction and
pharmacology training prior to prescribing these medications
and obtain a special DEA number that is necessary on all
prescriptions. Medication-assisted treatment is the beginning
of a life-long commitment to a drug and alcohol free lifestyle
that may require medication for months or years or may be a
part of life-long recovery.
NALTREXONE (VIVITROL)
• Naltrexone is an opioid receptor blocker
that prevents the euphoric eects and
impacts sedative eects of drugs such as
heroin, morphine or codeine.
• Naltrexone is typically given as a monthly
injection for treatment of alcohol or
opioid dependence, or it may be used
to prevent relapse following detox
from opioids.
• After receiving Naltrexone, using opioids
in large enough amounts to counter the
“blocking eects of the medication” can
result in overdose, respiratory arrest,
or death.
• Studies have shown statistically
signicant reduction in opioid cravings
following the use of Naltrexone.
• Currently, most private pay insurances
and all managed care organizations
(MCOs) under WV Medicaid cover the
cost of Vivitrol. If a patient does not have
insurance, the manufacturer of Vivitrol
has a co-pay savings program to assist
with the cost of co-pays and provide
assistance to help cover the cost of
the medication.
• Best practices with Naltrexone include
counseling as well as 12-step support
groups as an integral part of this form of
medication-assisted treatment for chance
of a successful recovery.
• In addition, studies have shown that
problem drinkers have signicantly fewer
drinking days and increased abstinence
when treated with Naltrexone for
alcohol dependency.
BUPRENORPHINE (SUBOXONE)
• Medication-assisted treatment of opioid
dependence can also use buprenorphine
combined with naloxone (best known
by the brand name Suboxone) as part
of a complete treatment plan including
counseling, 12-step support groups and
other psychosocial support therapy.
Buprenorphine combined with naloxone
is typicall
y administered via either a
sublingual strip or pill and taken orally.
• As with all forms of medication-assisted
treatment, dosage varies between
patients. The goal of the medication is
to manage the withdrawal symptoms
and cravings for heroin and other opioids
while fostering recovery from the brain
disease of addiction.
BUPRENORPHINE (BUPRENEX)
• Medication-assisted treatment of opioid
dependence can also use buprenorphine
without naloxone. This medication is
relatively safe to use in the treatment
of pregnant women. Talk with the
healthcare provider about the risks and
benets to the mother and the fetus prior
to treatment. This type of medication-
assisted treatment typically reverts
to use of another medication for MAT
about 6 weeks postpartum. As with all
other medication used with this model
of treatment, counseling and 12-step
support groups are an integral part of this
type of medication-assisted treatment.
METHADONE
• Methadone is a medication used in
medication-assisted treatment to help
people reduce or completely stop use
of heroin or other opioids and has
been used for MAT longer than any
other medication.
• As with all MAT medications, methadone
helps reduce cravings and withdrawal
symptoms from opioids for 24-48 hours.
This medication is long acting, meaning
it stays in the body and is eective for a
long period.
• Methadone is a full agonist, meaning
that it acts on the brain in the same way
as other opioids. The long-action of this
medication, combined with counseling
and 12-step support groups, fosters
recovery by eliminating the highs and
lows of drug use as well as eliminating
the withdrawal symptoms and cravings
for other opioids.
ANTIDOTE MEDICATION
NALOXONE (NARCAN)
• This medication is used, along with
emergency medical treatment, to reverse
suspected opioid overdose by reversing
the eects of the opioid taken to excess.
• Naloxone is given by injection, either IV
(into the vein) or into muscle or fat, or, in
a nasal mist.
• Naloxone reverses eects of opioids
(narcotics, heroin, etc.).
• Since this medication reverses the eects
of opioids, the person who overdosed will
experience sudden withdrawal symptoms
following the administration of naloxone.
• Naloxone is available by prescription
and may be available over the counter in
some locations.
Sources: Seneca Health Services, Inc./
Crosswinds and Mary Aldred-Crouch,
MSW, MPH, LICSW, MAC, AADC,
Clinical Consultant.
Contact your
insurance company to nd
out what providers and treatments
are available to you. If you do not
have insurance or have questions
about treatment services,contact
the Substance Abuse and
Behavioral Health Helpline at
1-844-HELP4WV.
RESOURCE
33

FMRS MOTHER PROGRAM
(304) 256-7146 or (304) 256-7100
RESOURCES
ACT UNIT VALLEY HEALTH
100 Crosswinds Drive, Fairmont, WV
(304) 363-2228
Substance abuse treatment center
that focuses on detoxication.
Residential program that lasts up to
30 days (sometimes 45, depending on
circumstances). Oers services for both
adolescents and adults.
ALCOHOLICS ANONYMOUS (AA)
Toll free: 1-877-331-3394
Call to nd a local meeting.
AMITY CENTER
1011 Mission Drive, Parkersburg, WV
(304) 465-1781
Residential drug and alcohol treatment
center for adult men and women. Services
include but are not limited to: Addiction
Counseling, Crisis Stabilization Program,
Court-Directed Treatment, Drug/Urine
Screens, AA, NA, and Al-Anon.
APPALACHIAN TEEN CHALLENGE
(304) 384-9074 or (304) 384-3307
1651 Unity Road, Princeton, WV
Christian residential program for men 18
and older. Provides spiritual counseling
with residents who have substance abuse
or anger management issues. Contact the
center for fees.
CELEBRATE RECOVERY
A Christian-centered recovery program
Rhema Christian Center
3584 Davis Stuart Road, Lewisburg WV
(304) 645-6999
34 | Greenbrier County Care Coalition
This program is where men and women can
nd support in overcoming behaviors or
habits that are potentially life-controlling
including addiction, co-dependency, grief
and other issues. Open meetings and small
group share are Thursdays at 6 p.m.
CHARLESTON TREATMENT CENTER
2157 Greenbrier Street, Charleston, WV
(304) 344-5924
The Charleston Treatment Center
provides medically supervised methadone
maintenance and Suboxone (buprenorphine)
detox treatment to individuals who are
attempting to overcome an addiction to or
dependence upon heroin or other opioids.
CHESTNUT RIDGE
930 Chestnut Ridge Road, Morgantown, WV
(304) 598-6364
Services include inpatient hospitalization
and detoxication, partial hospitalization,
intensive outpatient, outpatient individual
and group therapy, and an opioid specic
treatment program.
CROSSWINDS CENTER
Seneca Health Services, Inc.
414 Industrial Park Road, Maxwelton, WV
www.shsinc.org
(304) 497-2850
Inpatient services including 5-10 day
detoxication services and crisis
stabilization are provided at Crosswinds.
Detox services for pregnant woman and
referrals for after-care and rehab are
also available.
FMRS HEALTH SYSTEMS, INC.
(MAIN OFFICE)
101 South Eisenhower Drive
Beckley, WV 25801
(304) 256-7100
FMRS CRISIS STABILIZATION PROGRAM
101 South Eisenhower Drive
Beckley, WV 25801
(304) 256-7100 or 1-888-523-6437
Oers opioid, alcohol and benzodiazepine
detoxication, intensive group and
individual therapy, supportive group and
individual counseling, as well as linkage
and referrals for after care when
appropriate. The average length of stay is
ve to seven days for psychiatric symptoms
and six days for detoxication admissions.
Must be 18 or older with mental health
or substance abuse diagnosis. Pregnant
women will not be admitted.
FMRS LEARN PROGRAM
(304) 256-7144 or (304) 256-7100
Twelve week residential treatment program
for men ages 18 and older with substance
abuse issues. The program provides a
structured environment, individual and
group counseling daily. The program
includes a complete assessment, detox if
needed and treatment for any co-occurring
physical or mental health disorders. When
a wait list is in place, preference is given to
men who are injecting drugs of abuse.
A six-month residential treatment program
is available for women age 18 and older
with substance abuse issues. The program
provides a structured environment with
individual and group counseling daily. The
program includes a complete assessment,
detox if needed and treatment for any
co-occurring physical or mental health
disorders. Often women referred to the
MOTHER Program have children who may
need to accompany them to the residential
program. When a wait list for admission is
in place, preference is given to women who
are injecting drugs of abuse.
FMRS TURNING POINT PROGRAM
(304) 252-6783
This program oers a 90 day residential
program for women 18 and older who
are pregnant or postpartum (have a baby
a year old or less) who have substance

use disorders. Women may either slowly
taper o opioids if that is the drug of choice,
or to use Medication Assisted Treatment
(Subutex).
FRUITS OF LABOR, INC.
(304) 438-7425
fruitso[email protected]
www.fruitsoaborinc.com
Fruits of Labor is a Culinary and Agriculture
Educational Center that provides a unique
American Culinary Federation (ACF) Quality
Farm-to-Table Training Program. This
statewide opportunity provides various
national and state certicates as well as
continuing education hours through the
ACF while working with strengthening and
uplifting the whole person. Fruits of Labor’s
Seeds of Recovery Program is for those in
recovery from addiction with preference
to those enrolled in WV Drug Court/Court
Systems.
GREENBRIER CARE FAMILY PRACTICE
167 Kate’s Mountain Road
White Sulphur Springs, WV 24986
(304) 536-8018
Psychological services are oered.
MID-OHIO VALLEY FELLOWSHIP HOME
1030 George Street, Parkersburg, WV
(304) 485-3341
Sponsor to assist through 12 step program.
AA/NA meetings. 18 and older.
NARCOTICS ANONYMOUS (NA)
Toll free: 1-888-328-2518
Call to nd a local meeting.
NATIONAL INSTITUTE ON DRUG ABUSE
www.drugabuse.gov
Provides various drug fact sheets
and resources.
PARCWEST
1420 Washington Avenue, Huntington, WV
Main number (304) 697-1277
Intake 1: (304) 525-1522, ext. 2546
Intake 2: (304) 525-7851, ext. 1193
Hotline 1: (800) 642-3434
Hotline 2: (304) 525-7851, ext. 1193.
Short-term residential treatment program
(30 days or less) that provides services to
persons with co-occurring mental health
and substance abuse disorders. Payment
assistance available (check with facility) and
program accepts Medicaid, private insurance,
and self-pay. Sliding fee scale available.
PYRAMID COUNSELING, LLC
pyramidcounselingllc.com
(304) 645-5558
Toll free: (877) 588-0200
Valley Medical Building
3738 Davis Stuart Road, Lewisburg, WV
Services available for addiction, mental
health, outpatient, intensive outpatient and
support group.
RENAISSANCE PLACE
1853 8th Avenue Huntington, WV 25703
(304) 525-7851, ext. 4503
Drug and alcohol rehabilitation center
with a primary focus on substance abuse
treatment. Facility provides outpatient care
and buprenorphine services to the public.
There are special groups and programs
for persons with co-occurring mental and
substance abuse disorders, pregnant and
postpartum women, and criminal justice
groups. Special language services provided
include assistance for hearing impaired.
Payments via Medicaid, Medicare, private
insurance, and military insurance are
accepted. Payment assistance is oered
by way of sliding fee scale and case-by-
case basis (check with facility for specics)
treatment, and hospital inpatient options for
those who enroll.
STORM HAVEN TRANSITIONAL HOME
P.O. Box 130, Raleigh, WV
(304) 253-4879
Structured, sober living environment
designed to help those who are serious
about recovery from addiction.
SUBSTANCE ABUSE AND MENTAL HEALTH
SERVICES ADMINISTRATION (SAMHSA)
ndtreatment.samhsa.gov
Organization whose goal is to reduce the
impact of substance abuse and mental
illness on America’s communities. By using
the link, one can nd a treatment facility
anywhere in the U.S.
WVDHHR COMPREHENSIVE BEHAVIORAL
HEALTH CENTERS DIRECTORY
bit.ly/BehavioralHealthCenterDirectory
Lists behavioral health centers and their
respective contact information.
WV PEER RECOVERY RESOURCES GUIDE
bit.ly/PeerRecoveryWV
Lists admission criterion for various state
substance abuse programs.
WV PRESCRIPTION DRUG ABUSE
1-866-987-8488
Prescription Opioid and Heroin Awareness Toolkit | 35
NEW BEGINNINGS WOMEN’S
RESIDENTIAL TREATMENT
202 Columbia Street, Fairmont, WV
1-866-426-7444
Long-term residential treatment program
(30 days or more) that oers substance
abuse services to women. Accepts Medicaid,
private insurance and self-pay.
OAKHURST OUTREACH, INC.
(304) 536-1981
Oakhurst Outreach provides WV women a
safe, clean and secure home as they explore,
learn and create a new, substance free and
satisfactory lifestyle.
SENECA HEALTH SERVICES, INC.
804 Industrial Park Road, Maxwelton, WV
(304) 497-0500
Outpatient substance abuse counseling,
psychiatric evaluation, and medication
management. Accepts insurance, Medicaid,
Medicare, and income based self-pay.
SOUTHERN WV FELLOWSHIP HOME
201 Woodlawn Avenue, Beckley, WV
(304) 253-1411
Treatment facility in Beckley that specializes
in substance abuse and mental health
services. They provide residential short-
term treatment, residential long-term

Committee under the
Greenbrier County Family Resource Network
Alternative Solutions, PLLC
Burlington United Methodist
Family Services, Inc.
Celebrate Recovery
Children’s Home Society
City of Lewisburg
Communities in Schools of
Greenbrier County
Crosswinds Center
Day Report Center
Drug Free Mother Baby Program
Family Refuge Center
Fritz’s Pharmacy
Greenbrier County Chamber
of Commerce
Greenbrier County Committee
on Aging
Greenbrier County Elder Abuse
Awareness Committee
Greenbrier County Family
Resource Network
Greenbrier County Community
Corrections
PARTNERS INCLUDE:
Greenbrier County Health Department
Greenbrier County Homeland Security
and Emergency Management
Greenbrier County Probation
Greenbrier County Prosecuting
Attorney Oce
Greenbrier County Schools
Greenbrier County Sheri’s Oce
Greenbrier Medical Arts Pharmacy
Home Care Plus
Lewisburg Police Department
Mountain Health Trust/Maximus
Oakhurst Outreach, Inc.
Rainelle Medical Center
Rhema Christian Center
Robert C. Byrd Clinic
Town of Rainelle
Visability
WV Military Family
Assistance Center
WVU Extension
Young Life Greenbrier County
Additional support provided by:
