
1
U.S. Department of Health & Human Services
Centers for Medicare & Medicaid Services
Center for Medicare & Medicaid Innovation
Patient Care Models Group
7500 Security Boulevard
Baltimore, MD 21244
Guiding an Improved Dementia Experience
Request for Applications
Version: 1
Last Modified: November 7, 2023
2
Contents
MODEL SUMMARY ................................................................................................................................. 4
BACKGROUND ........................................................................................................................................ 7
SCOPE AND DURATION ......................................................................................................................... 10
GUIDE PARTICIPANTS ........................................................................................................................... 11
Participation Requirements ........................................................................................................... 13
Application .................................................................................................................................... 15
GUIDE Model Eligibility Criteria ..................................................................................................... 15
Program Integrity Screening ......................................................................................................... 16
Participant Withdrawal Policy....................................................................................................... 17
BENEFICIARY ELIGIBILITY AND BENEFICIARY ALIGNMENT .................................................................... 18
Overview ....................................................................................................................................... 18
Beneficiary Eligibility ..................................................................................................................... 18
Beneficiary Outreach and Engagement ......................................................................................... 19
Beneficiary Alignment ................................................................................................................... 20
Model Tiers ................................................................................................................................... 22
CARE DELIVERY ..................................................................................................................................... 24
Care Delivery Requirements .......................................................................................................... 24
Care Team Requirements .............................................................................................................. 26
Care Navigator Training ................................................................................................................ 27
Care Delivery Reporting ................................................................................................................ 28
PERFORMANCE MEASUREMENT ........................................................................................................... 29
PAYMENT DESIGN ................................................................................................................................. 32
Dementia Care Management Payment ......................................................................................... 33
Health Equity Adjustment ............................................................................................................. 36
Performance-Based Adjustment .................................................................................................... 37
Respite Payment ........................................................................................................................... 42
Payment Examples ........................................................................................................................ 45
Infrastructure Payment ................................................................................................................. 47
HEALTH EQUITY STRATEGY ................................................................................................................... 50
Health Equity Plan Requirement ................................................................................................... 50
Health Equity Data Collection Requirement .................................................................................. 51
3
LEARNING SYSTEMS STRATEGY............................................................................................................. 52
DATA ..................................................................................................................................................... 52
Data Reporting Requirements ....................................................................................................... 52
Data Sharing ................................................................................................................................. 53
PARTICIPANT MONITORING, AUDITING, AND TERMINATION STRATEGY ............................................. 54
EVALUATION ......................................................................................................................................... 54
AUTHORITY TO TEST THE MODEL ......................................................................................................... 54
Authority to Test the Model .......................................................................................................... 54
Waiver and OIG Safe Harbor Authority ......................................................................................... 55
Benefit Enhancement and Beneficiary Engagement Incentive ...................................................... 55
MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) ALTERNATIVE PAYMENT MODEL (APM) AND
ADVANCED APM STATUS ...................................................................................................................... 56
PROGRAM OVERLAPS AND SYNERGIES ................................................................................................. 56
Overlaps with Shared Savings Program and Innovation Center ACO Models ................................ 57
Overlaps with the BPCI Advanced and Comprehensive Care for Joint Replacement (CJR) Models . 57
Overlaps with Innovation Center models that have care management payments ........................ 58
Appendix A: Participant Application Guidance and Questions ............................................................. 59
Appendix B: Care Delivery Requirements ............................................................................................. 67
Appendix C: Example Patient Assessment and Alignment Form ........................................................... 76

4
Model Summary
This Request for Applications (RFA) introduces the Guiding an Improved Dementia Experience (GUIDE)
model, a new Center for Medicare and Medicaid Innovation (Innovation Center) model from the Centers
for Medicare & Medicaid Services (CMS). The GUIDE Model will test whether providing an alternative
payment methodology for participating dementia care programs to deliver a package of care
management and coordination, caregiver education and support, and GUIDE Respite Services to
Medicare beneficiaries with dementia and their caregivers
1
reduces expenditures while preserving or
enhancing quality of care.
The GUIDE Model is designed to enhance quality of care by improving quality of life for people with
dementia and reducing burden and strain on their caregivers. It is expected to reduce Medicare and
Medicaid expenditures primarily by preventing or delaying long-term nursing home stays, and
secondarily by reducing hospital, emergency department, and post-acute care utilization.
The GUIDE Model is a key deliverable from President Biden’s April 2023 Executive Order on Increasing
Access to High-Quality Care and Supporting Caregivers, as well as key goals of the National Plan to
Address Alzheimer’s Disease.
Key Model Elements:
• Scope and Duration: The GUIDE Model will be an 8-year voluntary model that is offered
na
tionwide, and will run from July 1, 2024 through June 30, 2032 (“Model Performance
Period”). The GUIDE Model will have two participant tracks, one for established dementia care
programs and one for new dementia care programs. The first performance year for the
established program track will begin on July 1, 2024. The new program track will have a one-
year pre-implementation period that begins on July 1, 2024, and its first performance year will
begin on July 1, 2025.
• Participants: GUIDE Participants will be Medicare Part B-enrolled providers or suppliers
(excluding durable medical equipment (DME) and laboratory suppliers) that establish Dementia
Care Programs (“DCPs”) to provide ongoing, longitudinal care to people with dementia (“GUIDE
Participant”). A GUIDE Participant must participate in the GUIDE Model under a single, Medicare
Part B-enrolled Taxpayer Identification Number (TIN) that is eligible to bill for Medicare
Physician Fee Schedule (PFS) services. A GUIDE Participant must meet the care delivery
requirements described in the “Care Delivery” section of this RFA but may choose to partner
with other organizations, including both Medicare-enrolled providers and suppliers and non-
Medicare enrolled entities, such as community-based organizations, to meet these
requirements.
1
For purposes of the GUIDE Model, the term “caregiver” is defined as a relative, or an unpaid nonrelative, who
assists the beneficiary with activities of daily living and/or instrumental activities of daily living. Depending on the
beneficiary’s need, the assistance may be episodic, daily, or occasional.

5
• Beneficiary Eligibility and Beneficiary Alignment: Eligible beneficiaries will be community-
dwelling
2
Medicare FFS beneficiaries, including beneficiaries dually eligible for Medicare and
Medicaid, who have dementia. Beneficiaries will be aligned to GUIDE Participants through a
voluntary alignment process in which they are informed about the GUIDE Model and consent to
receive services from a specific GUIDE Participant. Aligned beneficiaries will maintain freedom of
choice with respect to their physicians or practitioners.
• Model Tiers: Beneficiaries will be assigned to one of five model tiers based on the complexity of
their needs, and, if applicable, their caregiver needs. Model services, care intensity, and
payment will vary by model tier. GUIDE Participants must re-assess each beneficiary at least
once per year, and CMS may re-assign beneficiaries to a different model tier based on the
results of the re-assessment.
• Care Delivery: The GUIDE care delivery approach includes 1) a standardized package of services
that GUIDE Participants must provide to beneficiaries and their caregivers (as applicable to
individual beneficiary and caregiver needs) (“GUIDE Care Delivery Services”); 2) an
interdisciplinary care team to deliver these services; and 3) a standardized training requirement
for care navigators who are part of the interdisciplinary care team. GUIDE Care Delivery Services
encompass nine care delivery domains: comprehensive assessment, care planning, ongoing
monitoring and support, medication reconciliation and management, 24/7 access to a care team
member or helpline, care coordination and transitional care management, referrals and
coordination for services and supports, caregiver education and support, and GUIDE Respite
Services. The interdisciplinary care team must include, at a minimum, a “care navigator,” and a
clinician with “dementia proficiency” who is eligible to bill Medicare Part B evaluation and
management services (E/M).
3
The terms “care navigator” and “dementia proficiency” are
defined in the section titled “Care Team Requirements.”
• Performance Measurement: CMS plans to measure GUIDE Participant performance on five
performance measures, including quality, patient experience, utilization, and cost metrics: Use
of High-Risk Medications in Older Adults; Quality of Life Outcome for People with Neurological
Conditions; Caregiver Burden; Total Per Capita Cost; and Long-Term Nursing Home Stay rate.
The caregiver burden and long-term nursing home stay rate are new metrics that will be
developed for use in the GUIDE Model.
• Per Beneficiary Per Month Payment: GUIDE Participants will be able to bill Medicare for a per
beneficiary per month Dementia Care Management Payment (“DCMP”). CMS will pay the DCMP
2
For the purposes of the GUIDE Model, the term “community-dwelling” is defined as living in a personal home,
assisted living facility, group home, or other community setting. A beneficiary will still be considered community-
dwelling for the purposes of the model if they are admitted to an acute care hospital or receive post-acute care in
skilled nursing facility. A beneficiary will no longer be considered community-dwelling if the person becomes a
long-term nursing home resident, defined as having a nursing home stay that is not covered under the Medicare
skilled nursing facility benefit.
3
See “Care Delivery” section for more detailed criteria for the care navigator role and the definition of “dementia
proficiency”.
6
to GUIDE Participants for furnishing the GUIDE Care Delivery Services to aligned beneficiaries
(with the exception of GUIDE Respite Services, which will be paid for under a separate
payment). The GUIDE Participant’s DCMP amount will depend on the aligned beneficiary’s
model tier; each of the five model tiers will have a different DCMP rate. The DCMP will be
adjusted by a performance-based adjustment tied to the five model performance metrics, as
well as a health equity adjustment. The health equity adjustment will increase the DCMP paid to
the GUIDE Participant for low-income aligned beneficiaries from underserved communities and
it will decrease the DCMP paid to the GUIDE Participant for higher income aligned beneficiaries
from more advantaged communities. The health equity adjustment is intended to provide an
incentive for GUIDE Participants to deliver care to beneficiaries from underserved communities.
The GUIDE Model is not a total cost of care model and GUIDE Participants may continue to bill
for all services not included in the DCMP under traditional Medicare FFS.
• Payment for GUIDE Respite Services: GUIDE Participants will be able to bill the Innovation
Center for up to $2,500 per aligned beneficiary per year for GUIDE Respite Services. Only certain
aligned beneficiaries will be eligible for GUIDE Respite Services (see Requirements for Aligned
Beneficiaries to be Eligible to Receive GUIDE Respite Services under the “Respite Payment”
section of this RFA). GUIDE Participants must offer in-home GUIDE Respite Services but may also
choose to offer adult day center and facility-based respite.
• Health Equity: To address disparities in dementia care, GUIDE Participants will be required to
develop and implement a Health Equity Plan that identifies disparities in outcomes in their
patient populations and strategies to reduce these disparities over the course of their
participation in the GUIDE Model. GUIDE Participants will also be required to collect and report
data on beneficiaries’ sociodemographic characteristics and health-related social needs (though
beneficiaries will always have the option to opt out of sharing their data). This data will help
GUIDE Participants identify and address disparities within their patient population and track
their progress towards health equity goals over time.
• Data Reporting and Sharing: In addition to the sociodemographic and health-related social
needs data described above, GUIDE Participants will also be required to report quality and care
delivery data on an annual basis. This information will be used to assess GUIDE Participant
performance and inform the model evaluation. GUIDE Participants will also receive data from
CMS, primarily in the form of a Data Dashboard. The Data Dashboard will provide GUIDE
Participants with an interactive, user-friendly interface for viewing claims-based utilization data
for their aligned beneficiaries, updated monthly, available and aggregated across the GUIDE
Participant’s entire aligned population.

7
Background
6.7 million Americans currently live with Alzheimer’s disease or another form of dementia, a number
that is projected to grow to nearly 14 million by 2060.
4
Despite the high prevalence of dementia—
roughly 11 percent of U.S. adults over the age of 65 and nearly 35 percent over the age of 85 have
dementia
5
—many people with dementia are not consistently receiving high quality, high value care.
People with dementia experience poor outcomes across an array of metrics, including high rates of
hospitalization, ED visits, and post-acute care utilization,
6,7
high rates of depression, behavioral and
psychological symptoms of dementia (BPSD),
8
and poor management of other co-occurring
conditions.
9,10
As the condition progresses, many people with dementia will need long-term services and
supports, including care in a nursing facility or home and community-based services.
With support and collaboration, primary care can play an important role in improving care delivered to
people with dementia, including providing person-centered care and coordinating across providers to
manage a person’s co-occurring conditions.
11
However, the primary care setting often lacks the
resources to independently provide the intensive services that people with dementia need—services
such as identifying and helping connect to services and supports, addressing behavioral symptoms, and
re-stabilizing after an acute health event.
Dementia not only affects quality of life for people with the disease—it also significantly impacts quality
of life for caregivers. Many caregivers for people with dementia, who are often Medicare beneficiaries
themselves, report high levels of stress and depression,
12
which negatively affect their overall health and
increase their risk for serious illness, hospitalization, and mortality.
13,14
Dementia also imposes a large
financial burden on beneficiaries and their families: out-of-pocket spending in the last five years of life,
including for long term services and supports, is higher for people with dementia compared to those
4
Alzheimer's Association. 2023 Alzheimer's Disease Facts and Figures.
https://www.alz.org/media/documents/alzheimers-facts-and-figures.pdf
5
Ibid.
6
Lin P-J, Fillit HM, Cohen JT, Neumann PJ, et al. Potentially avoidable hospitalizations among Medicare
beneficiaries with Alzheimer’s and related disorders. Alzheimer’s & Dementia. January 2013. 9(1): 30-38.
7
Feng Z, Coots LA, Kaganova Y and Wiener JM. Hospital and ED Use Among Medicare Beneficiaries with Dementia
Varies by Setting and Proximity to Death. Health Affairs. April 2014. 33(4).
8
Lyketsos, CG, Lopez O, Jones B, et al. Prevalence of Neuropsychiatric Symptoms in Dementia and Mild Cognitive
Impairment: Results from the Cardiovascular Health Study. JAMA. September 2002. 288(12): 1475-1483.
9
Zhao Y, Kuo T-C, Weir S, et al. Healthcare costs and utilization for Medicare beneficiaries with Alzheimer’s. BMC
Health Services Research. May 2008.
10
Thorpe CT, Thorpe JM, Kind AJH, et al. Receipt of Diabetes Monitoring in Older Adults with Co-Morbid Dementia.
Journal of the American Geriatric Society. April 2012. 60(4): 644-651.
11
Boustani M, Schubert C, and Sennour Y. The challenge of supporting care for dementia in primary care. Clin
Interv Aging. December 2007. 2(4).
12
Teri L, McKenzie G, Logsdon RG, McCurry SM, Bollin S, et al. Translation of two evidence-based programs for
training families to improve care of persons with dementia. Gerontologist. 2012. 52: 452–459.
13
Schubert CC, Boustani M, Callahan CM, Perkins AJ, Hui S, et al. Acute care utilization by dementia caregivers
within urban primary care practices. Journal of General Internal Medicine. 2008: 23: 1736–1740.
14
Schulz R, Martire LM. Family caregiving of persons with dementia: prevalence, health effects, and support
strategies. American Journal of Geriatric Psychiatry. 2004. 12: 240–249.

8
without dementia ($61,522 vs. $34,068), and people with dementia end up spending a significantly
higher share of their total family assets on care in the last five years of life (32% vs 11%).
15,16
All of these issues are exacerbated for certain racial and ethnic groups. Black and Hispanic populations
have a higher prevalence of dementia,
17,18
but they also are less likely to receive a timely diagnosis,
19
have more unmet needs,
20
are more likely to experience high caregiving demands, and spend a higher
share of their family assets on dementia care.
21,22,23, 24
Though much of the financial burden of dementia falls on beneficiaries and their caregivers through out-
of-pocket spending, dementia also drives higher costs for federal health care programs. Two recent
studies have estimated that, on average, a person with dementia will have an additional $12,000-
$15,700 in total Medicare costs and an additional $8,800-$31,000 in total Medicaid costs over the 5
years after diagnosis.
25,26
Driven by this evidence of the enormous burden that dementia imposes on individuals, families,
caregivers, and society at large, numerous federal groups and agencies have sought to identify
interventions that can improve care and outcomes for people with dementia and their caregivers. Many
of these federal partners have identified care coordination and caregiver education and support
programs like the GUIDE Model as promising interventions. For example, the GUIDE Model is consistent
with recommendations in the National Plan to Address Alzheimer’s Disease, which is the nation’s
roadmap for addressing dementia that includes input from ASPE, OASH, NIA, CMS, CDC, ACL, HRSA,
15
Hudomiet P, Hurd M, Rohwedder S. The relationship between lifetime out-of-pocket medical expenditures,
dementia, and socioeconomic status in the US. The Journal of the Economics of Aging. 2019. 14.
16
Kelley AS, McGarry K, Gorges R, Skinner JS. The Burden of Health Care Costs for Patients with Dementia in the
Last 5 Years of Life. Annals of Internal Medicine. November 2015.
17
Lennon, et al. Black and white individuals differ in dementia prevalence, risk factors, and symptomatic
presentation. Alzheimer’s and Dementia. 2021.
18
Lines, LM and Wiener JM. Racial and Ethnic Disparities in Alzheimer’s Disease: A Literature Review. Office of the
Assistant Secretary for Planning and Evaluation (ASPE). 31 January 2014.
19
Gianattasio KZ, Prather C, Glymour MM, et al. Racial disparities and temporal trends in dementia misdiagnosis
risk in the United States. Alzheimer’s & Dementia. December 9, 2019.
20
Black BS, Johnston D, Leoutsakos J, et al. Unmet needs in community-living persons with dementia are common,
often non-medical and related to patient and caregiver characteristics. International Psychogeriatrics. November
2019. 31(11).
21
Friedman EM, Shih RA, Langa KM, Hurd MD. US prevalence and predictors of informal caregiving for dementia.
Health Affairs Project Hope. 2015. 34(10):1637–41.
22
Lines LM, Wiener JM. Racial and Ethnic Disparities in Alzheimer’s Disease: A Literature Review. Report prepared
for Office of Disability, Aging and Long-Term Care Policy in the Office of the Assistant Secretary for Planning and
Evaluation. February 2014. Contract #HHSP23320100021WI.
23
Hudomiet et al. (2019).
24
Kelley et al. (2015).
25
White L, Fishman P, Basu A, et al. Medicare expenditures attributable to dementia. Health Services Research.
2019. 54: 773-781.
26
Coe NB, White L, Oney M, et al. Public spending on acute and long-term care for Alzheimer's disease and related
dementias. Alzheimer's & Dementia. 20 January 2022.

9
AHRQ, SAMHSA, FDA, IHS, and ACF
27
and is informed by the Advisory Council on Alzheimer’s Research,
Care, and Services. The National Plan recommends that CMS explore the effectiveness of new models of
care for people with Alzheimer’s disease and related dementias, and that CMS implement and evaluate
care coordination models for people with dementia.
28
It is also consistent with a 2021 National Academies for Science, Engineering, and Medicine (NASEM)
consensus report recommending that collaborative dementia care models and multi-component
caregiver support programs should be implemented and evaluated in multiple and varied real-world
settings.
29
The GUIDE Model also builds on lessons learned from the Department of Veteran Affairs (VA) Program
of General Caregiver Support Services (PGCSS), which has experience implementing numerous caregiver
education and support interventions, including caregiver skills trainings, individual and group counseling,
peer support mentoring, and respite services.
30
The GUIDE Model is consistent with Executive Order 14095 signed on April 18, 2023, “Increasing Access
to High-Quality Care and Supporting Caregivers”, which directed the Secretary of Health and Human
Services to “consider whether to select for testing by the Center for Medicare and Medicaid Innovation
an innovative new health care payment and service delivery model focused on dementia care that
would include family caregiver supports such as respite care.”
Finally, the GUIDE Model builds on a substantial body of evidence from both previous CMS models and
demonstration projects and external, provider-based dementia care programs. Like the GUIDE Model,
these dementia care programs aimed to provide comprehensive, interdisciplinary care to people with
dementia and their caregivers, with the goal of improving the person and their caregiver’s quality of life
while reducing avoidable health care utilization and delaying or avoiding long-term nursing home stays.
Overall, there is evidence that dementia care programs improve beneficiary and caregiver experience of
care, increase self-reported caregiver efficacy, and lower caregiver stress.
31,32
27
Office of the Assistant Secretary for Planning and Evaluation (ASPE), Office of the Assistant Secretary for Health
(OASH), National Institute on Aging (NIA), Centers for Medicare & Medicaid Services (CMS), Centers for Disease
Control and Prevention (CDC), Administration for Community Living (ACL), Health Resources and Services
Administration (HRSA), Agency for Healthcare Research and Quality (AHRQ), Substance Abuse and Mental Health
Services Administration (SAMHSA), Food and Drug Administration (FDA), Indian Health Service (IHS), and
Administration for Children and Families (ACF).
28
National Plan to Address Alzheimer’s Disease: 2022 Update. U.S. Department of Health and Human Services.
https://aspe.hhs.gov/sites/default/files/documents/59cefdd628581b48b2e389891a675af0/napa-national-plan-
2022-update.pdf
29
NASEM Committee on Care Interventions for Individuals with Dementia and Their Caregivers. 2021.
30
Factsheet: Department of Veterans Affairs Program of General Caregiver Support Services. March 2022.
https://www.caregiver.va.gov/pdfs/FactSheets/CSP_PGCSS_Fact_Sheet.pdf
31
NASEM Committee on Care Interventions for Individuals with Dementia and Their Caregivers. Meeting the
Challenge of Caring for Persons Living with Dementia and Their Care Partners and Caregivers: A Way Forward.
Washington, DC: The National Academies Press. 2021.
32
Agency for Healthcare Research and Quality. Care Interventions for People with Dementia and Their Caregivers.
Comparative Effectiveness Review Number 231. August 2020.

10
CMS has previously tested five dementia care models or demonstrations: four dementia care projects
funded through the Innovation Center’s Health Care Innovation Awards (HCIA),
33
and a multi-site
Medicare demonstration.
34
According to a synthesis of evaluation results conducted by the Innovation
Center’s Research and Rapid Cycle Evaluation Group (RREG),
35
key findings across the five projects were
that: 1) access to dementia care resources improved beneficiaries’ and caregivers’ experience of care; 2)
caregivers reported increased efficacy in their caregiving abilities and lower stress; 3) there was a
significant reduction in long-term nursing home stays in one project; and 4) there were non-significant
reductions in Medicare expenditures, ED visits, and hospitalizations in several projects. The evaluation
followed beneficiaries during their period of enrollment in each project, which varied from 12 to 36
months on average.
The GUIDE Model is designed to investigate whether 1) defining a specific package of dementia care
services, 2) tiering the intervention intensity based on a person’s needs and targeting high-intensity care
to those with the greatest need, 3) providing access to GUIDE Respite Services, and 4) using a longer,
eight-year performance period (as compared to previous dementia care demonstrations) could improve
outcomes or our ability to detect improved outcomes.
Scope and Duration
The GUIDE Model will be an 8-year voluntary national model that is offered in all states, U.S. territories,
and the District of Columbia. The Model Performance Period will begin on July 1, 2024 and end on June
30, 2032. The GUIDE Model will have two participant tracks, one for established dementia care
programs and one for new dementia care programs. CMS will assign selected applicants to either the
established program track or the new program track. The purpose of the two tracks is to allow
established programs to begin their performance in the GUIDE Model on July 1, 2024, while giving
organizations that do not currently offer a comprehensive community-based dementia care program,
including safety net organizations, time and support to develop a new program. New program
development is intended to help to increase beneficiary access to specialty dementia care, particularly in
underserved communities.
The first performance year for the established program track will begin on July 1, 2024. The new
program track will have a one-year pre-implementation period that begins on July 1, 2024. The first
performance year for the new program track will begin on July 1, 2025 and both tracks will continue
through June 30, 2032. Table 1 illustrates the timeline for both tracks.
33
Health Care Innovation Awards. Centers for Medicare & Medicaid Services.
https://innovation.cms.gov/innovation-models/health-care-innovation-awards
34
Newcomer R, Miller R, Clay T, Fox P. Effects of the Medicare Alzheimer’s disease demonstration on Medicare
expenditures. Health Care Financ Rev. 1999. 20:45–65.
35
CMS Innovation Center. Dementia Care Projects: Synthesis of Evaluation Results, 1989-2020. December 2022.
https://innovation.cms.gov/data-and-reports/2022/dementia-care-synthesis-1989-2020

11
Table 1. Model Timeline for Established Program and New Program tracks
Nov. ’23-
Jan. ‘24
July 2024-
June 2025
July ’25-
June ‘26
July ’26-
June ‘27
July ’27-
June ‘28
July ’28-
June ‘29
July ’29-
June ‘30
July ’30-
June ‘31
July ’31-
June ‘32
Established
Program
Track
Application
Period
Performance
Year (PY) 1
PY 2 PY 3 PY 4 PY 5 PY 6 PY 7 PY 8
New
Program
Track
Application
Period
Pre-
Implementation
(PI) Period
PY 1 PY 2 PY 3 PY 4 PY 5 PY 6 PY 7
The application period will close on January 30, 2024. Applicants will be notified as to whether they
have been selected for participation in the GUIDE Model in Spring 2024. Onboarding for all selected
GUIDE Participants will take place in Spring 2024 and the GUIDE Model will begin on July 1, 2024.
GUIDE Participants
A GUIDE Participant will be a Medicare Part B-enrolled provider or supplier, excluding DME and
laboratory suppliers, that establishes a DCP to provide ongoing, longitudinal care to people with
dementia. The GUIDE Participant must participate under a single, Medicare Part B-enrolled Taxpayer
Identification Number (TIN) that is eligible to bill under the PFS.
The GUIDE Participant will be identified by a single TIN that is used to bill for GUIDE Model services, plus
the National Provider Identifiers (NPIs) of individual Medicare-enrolled physicians and other non-
physician practitioners who have re-assigned their billing rights to the GUIDE Participant’s billing TIN.
The GUIDE Participant will be required to maintain this list of physicians and non-physician practitioners
(“GUIDE Practitioner Roster”) and keep it up to date throughout the course of the GUIDE Model, as it will
be used to determine who is eligible to bill for GUIDE Model payments.
Contracting with Providers, Suppliers, and/or Organizations to Meet Care Delivery Requirements
A GUIDE Participant must meet the care delivery requirements described in the “Care Delivery” section
of this RFA. If a GUIDE Participant cannot meet the GUIDE care delivery requirements alone, the GUIDE
Participant may contract with one or more other providers, suppliers, or organizations, including both
Medicare-enrolled and non-Medicare enrolled entities, to meet the care delivery requirements. These
providers, suppliers, or organizations will be known as “Partner Organizations.”
For example, a multispecialty practice may contract with a Medicare enrolled home health agency to
have an occupational therapist, who is employed by the home health agency, provide some of the
required care delivery services.
In another example, a primary care physician may contract with a community-based memory care clinic,
that is not a Medicare enrolled provider, in order to provide some of the required care delivery services.
The GUIDE Participant will be expected to maintain a list of Partner Organizations (“Partner Organization
Roster”) and keep it up to date throughout the course of the GUIDE Model.
12
Both Medicare-enrolled and non-Medicare enrolled entities may contract with more than one GUIDE
Participant.
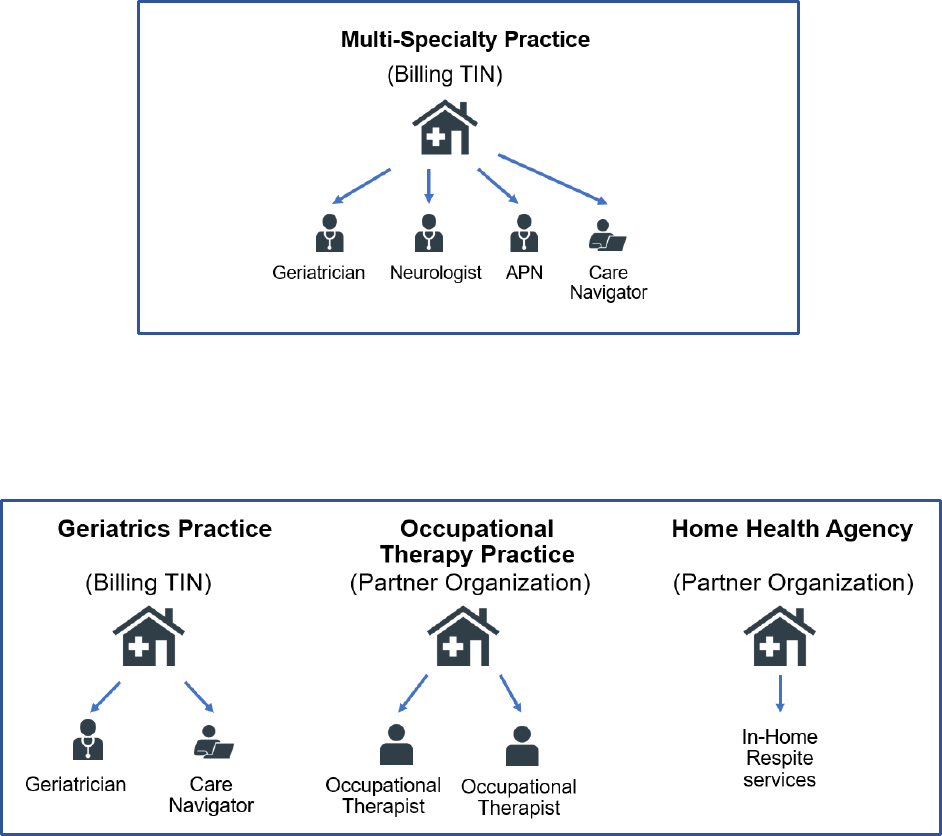
Examples of Dementia Care Programs
Example 1: A single Medicare provider forms a DCP
In this example, the DCP is established by a multi-specialty practice and model services are billed under
the practice’s TIN. The multi-specialty practice meets all care delivery requirements of the GUIDE Model,
including in-home GUIDE Respite Services, without a Partner Organization.
Example 2: A Medicare provider partners with several other Medicare providers to form a DCP
In example two, the DCP is established by a geriatrics practice, which is the GUIDE Participant. The
geriatrics practice partners with an occupational therapy practice and a home health agency to meet the
care delivery requirements of the GUIDE Model. The occupational therapy practice and the home health
agency are considered Partner Organizations within the DCP. All model services are billed by the GUIDE
Participant, in this case the geriatrics practice’s TIN, and all practitioners must re-assign their billing
rights to this TIN.

13
Example 3: Medicare-enrolled provider establishes a new Part B enrolled TIN to form a DCP
In example three, a home health agency establishes a new Medicare Part B-enrolled practice for the
purposes of participating in GUIDE. The Part B-enrolled practice is the GUIDE Participant, and model
services are billed under the practice’s TIN.
Example 4: A community-based provider partners with a primary care practice to form a DCP
In example four, a community-based memory care clinic, without a Part B-enrolled provider on staff,
partners with a Part B-enrolled primary care practice to meet the care delivery requirements of the
GUIDE Model. The Part B-enrolled primary care practice is the GUIDE Participant, and model services
are billed under the primary care practice’s TIN.
Participation Requirements
An applicant that is accepted to participate in the GUIDE Model will become a GUIDE Participant upon
execution of a Participation Agreement with CMS. The Participation Agreement will set forth the terms
of the GUIDE Model and each party’s obligations under the GUIDE Model.

14
GUIDE Participants must meet the following requirements, among others specified in the Participation
Agreement, throughout the performance period of their assigned track (e.g., July 1, 2024 - June 30, 2032
for the established program track and July 1, 2025 - June 30, 2032 for the new program track):
• Meet the interdisciplinary care team, care delivery, and training requirements, as described in
the Participation Agreement (see the “Care Delivery” section and appendix B of this RFA).
• Use an electronic health record platform that meets CMS and Office of the National Coordinator
for Health Information Technology (ONC) standards for Certified Electronic Health Record
Technology (CEHRT) as defined at 42 CFR 414.1305.
36
• The GUIDE Participant has the flexibility to provide most model services virtually or in-person (in
office or in the beneficiary’s home) but must conduct an initial home visit in-person for aligned
beneficiaries who have moderate to severe dementia.
• The GUIDE Participant is required to make available for eligible beneficiaries GUIDE Respite
Services in the beneficiary’s home. The GUIDE Participant has the option, but is not required to,
offer eligible beneficiaries GUIDE Respite Services at an adult day center or a facility that can
provide 24-hour care. More details regarding GUIDE Respite Services can be found in the
“Respite Payment” section of this RFA.
• Maintain an up-to-date GUIDE Practitioner Roster and Partner Organization Roster.
• Comply with all model reporting requirements, including care delivery, sociodemographic data,
and quality reporting.
GUIDE Participants in the new program track will be required to use the one-year pre-implementation
period, from July 1, 2024 to June 30, 2025, for program development, including hiring and training staff,
establishing program work flows and processes, developing provider networks, and building
relationships with community-based organizations and respite suppliers and providers, as applicable.
GUIDE Participants in the new program track will not be required to meet the GUIDE Model’s care
delivery, care team, and Certified Electronic Health Record Technology (CEHRT) requirements until two
months before the beginning of their first performance year (by May 1, 2025). GUIDE Participants in the
new program track will be required to submit baseline care delivery reporting, a Proposed GUIDE
Practitioner Roster and, if applicable, a Proposed Partner Organization Roster by May 1, 2025 to enable
CMS to verify that they have met these requirements. CMS will conduct a program integrity screening
based on the proposed rosters. CMS will terminate from the GUIDE Model any GUIDE Participants in the
new program track who fail to meet these requirements by May 1, 2025. GUIDE Participants, who
receive an infrastructure payment and are then terminated from the GUIDE Model under the provisions
of this paragraph, are required to re-pay the infrastructure payment to CMS (see “Infrastructure
Payment” section of this RFA).
Additional comprehensive participation requirements will be set forth in the Participation Agreement.
36
ONC has proposed to require USCDI Version 3 in certified health IT products by January 1, 2025. Participants will
be required to use certified health IT that has been updated to a required version of the United States Core Data
for Interoperability (USCDI) Version 3, where applicable for certified functionality required under the CEHRT
definition at 42 CFR 414.1305, by the deadline finalized by ONC.

15
Application
Application questions, including deadlines and contact information, can be found in Appendix A.
A
pplicants must submit all application materials via an online portal available on the GUIDE Model
website at https://innovation.cms.gov/innovation-models/guide
by the deadline. It is the responsibility
of the applicant to ensure that they include all required information in their application.
Applicants seeking to withdraw their application must submit an electronic withdrawal request to CMS
v
ia the following mailbox: GUIDEModelTea[email protected]ov. The request must be submitted as a PDF on
the organization’s letterhead and must be signed by a corporate official authorized to bind the
applicant. It should include: the applicant organization’s registered name; the organization’s primary
point of contact; the full and correct address of the organization; and a description of the nature of the
withdrawal.
GUIDE Model Eligibility Criteria
To be selected for participation in the GUIDE Model, applicants must first meet the eligibility criteria, as
d
escribed below. Then, if accepted, CMS will assign the selected applicants to either the established
program track or the new program track based on the information provided in the application.
CMS will accept applicants that meet eligibility requirements for either the established program track or
t
he new program track taking into consideration eligibility for the relevant track, the results of the
program integrity screening, model size considerations, and other reasons.
Established Program Track
To be eligible for the established program track, an applicant must:
• Be a legal entity formed under applicable state, federal, or Tribal law, that is authorized to
conduct business in each state in which it operates;
• Be a Medicare Part B enrolled provider or supplier (excluding DME and laboratory suppliers)
t
hat is eligible to bill under the Medicare Physician Fee Schedule at the time of application;
• Have a currently practicing interdisciplinary team at the time of model announcement that has
p
rovided at least 6 of the 9 care delivery domains described in the “Care Delivery” section, for at
least the past 12 months prior to the deadline for application submissions, to people living with
dementia;
• Submit the NPIs of the Medicare-enrolled physicians and non-physician practitioners who they
a
re proposing to provide services under the GUIDE Model (“Proposed GUIDE Practitioner
Roster”);
• If applicable, submit a proposed list of the Partner Organizations with whom they would like to
partner in order to meet the care delivery requirements of the GUIDE Model (“Proposed Partner
Organization Roster”); and

16
• Use an electronic health record platform that meets CMS and Office of the National Coordinator
for Health Information Technology (ONC) standards for Certified Electronic Health Record
Technology (CEHRT) as defined at 42 CFR 414.1305.
37
New program track
To be eligible for the new program track, an applicant must:
• Be a legal entity formed under applicable state, federal, or Tribal law, that is authorized to
conduct business in each state in which it operates;
• Attest that prior to execution of the Participation Agreement (in Spring 2024), it will have
established a single, Part B enrolled TIN that is eligible to bill under the Medicare Physician Fee
Schedule for the purposes of GUIDE Model participation;
• Either not provide comprehensive dementia care to people living with dementia at time of
application (defined as at least 6 of the 9 care delivery domains described in the “Care Delivery”
section, delivered by an interdisciplinary team), or provide comprehensive dementia care, but
have only done so for less than 12 months prior to the deadline for application submissions.
• Describe, in their application, plans to implement a dementia care program that include:
o
o
o
o
o
Strategies for staffing;
Development of program protocols and workflows;
Training;
Development of a provider network; and
Identifying a program director who will have primary accountability for implementing
the dementia care program.
Applicants do not need to have a Medicare Part B enrolled TIN that is eligible to bill under the PFS at the
time of application to the GUIDE Model, but if selected for participation, the applicant must have one
prior to execution of the Participation Agreement. Signed Participation Agreements will be due back to
CMS in Spring 2024.
Program Integrity Screening
CMS will conduct a Program Integrity (PI) screening of all applicants (including practitioners submitted
on an applicant’s Proposed GUIDE Practitioner Roster) and their Proposed Partner Organizations Roster
as part of the application review process. CMS may deny selection to an otherwise qualified applicant
based on information found during PI screening of the applicant or any other relevant individuals or
entities associated with the applicant. For Medicare enrolled providers, the PI review may include the
following, without limitation, with respect to the applicant and Medicare enrolled Partner
Organizations:
37
ONC has proposed to require USCDI Version 3 in certified health IT products by January 1, 2025. Participants will
be required to use certified health IT that has been updated to a required version of the United States Core Data
for Interoperability (USCDI) Version 3, where applicable for certified functionality required under the CEHRT
definition at 42 CFR 414.1305, by the deadline finalized by ONC.
17
• Confirmation of current Medicare enrollment status as relevant and history of adverse
e
nrollment actions;
• Identification of Medicare and Medicaid debt;
• Review of performance in, and compliance with the terms of, other CMS models, demonstration
programs, and initiatives;
• Review of compliance with Medicare and Medicaid program requirements;
• Review of billing history and any administrative audits, investigations, or other activities
conducted regarding suspicious billing or other potential program fraud and abuse; and
• Review of any administrative, civil, or criminal actions related to program integrity or other
fac
tors relevant to participation in an initiative involving Federal funds.
The PI review may include the following, without limitation, with respect to the non-Medicare enrolled
Partner Organizations:
• Confirmation of current licensure or certification with the state, in which they are providing
s
ervices;
• Review of any criminal actions of the organization and its leadership, including related to
p
rogram integrity or other factors relevant to participation in an initiative involving Federal
funds.
In addition, CMS may also screen parent organizations to support an informed selection process and
i
dentify business practice, solvency, and program integrity concerns. Information evaluated may include,
but is not limited to: ownership, executive leadership, and care delivery experience.
If an applicant is selected for the new program track, CMS will conduct an additional program integrity
s
creening of the applicant’s Proposed GUIDE Practitioner Roster and Proposed Partner Organization
Roster when this information is submitted by the May 1, 2025 deadline as explained above under
“Participation Requirements”.
CMS will conduct program integrity screenings throughout the application period, after selecting
p
articipants, and during the performance period, and may deny or terminate participation in the GUIDE
Model based on the results of a program integrity screening or other information obtained regarding an
individual’s or entity’s history of program integrity issues at any point during or after the application and
selection processes.
Participant Withdrawal Policy
The GUIDE Participant may terminate its participation in the GUIDE Model upon advance written notice
t
o CMS, which must specify the effective date of termination. The GUIDE Participant must provide
advance written notice at least 180 days prior to the effective date of termination. Until the effective
date of termination, the GUIDE Participant must continue to provide model services to aligned
beneficiaries and may not accept the voluntary alignment of new beneficiaries. The GUIDE Participant
must also notify its aligned beneficiaries of its withdrawal from the GUIDE Model.

18
Beneficiary Eligibility and Beneficiary Alignment
Overview
The GUIDE Model is designed to serve community-dwelling
38
Medicare FFS beneficiaries, including
beneficiaries dually eligible for Medicare and Medicaid, who have dementia. For the purposes of the
GUIDE Model, a caregiver will be defined as a relative, or unpaid nonrelative, who assists the beneficiary
with activities of daily living
39
and/or instrumental activities of daily living.
40
Depending on the
beneficiary’s need, the assistance may be episodic, daily, or occasional.
The GUIDE Participant will develop provider networks and conduct outreach and engagement to recruit
b
eneficiaries for the GUIDE Model. GUIDE Participants in the established program track are required to
offer the opportunity to voluntarily align to their DCP to all beneficiaries with dementia to whom they
already provide dementia care services. CMS will also employ several outreach strategies to supplement
GUIDE Participants’ beneficiary recruitment activities (see “Beneficiary Outreach and Engagement”
section below for more detail).
The GUIDE Model will use a voluntary alignment process for aligning beneficiaries to GUIDE Participants.
Th
e beneficiary will learn about the GUIDE Model through a GUIDE Participant’s recruitment activities or
CMS’s outreach strategies and the beneficiary will have to consent to receive services from a specific
GUIDE Participant to be aligned to that GUIDE Participant. Even after a beneficiary has opted in and
been aligned to a GUIDE Participant, the GUIDE Model does not impact or restrict a beneficiary’s ability
to choose to receive health services from any provider or supplier.
Beneficiary Eligibility
A beneficiary must meet the following criteria to be eligible for voluntary alignment to a GUIDE
P
articipant:
• Has dementia, as confirmed by attestation from a clinician on the GUIDE Participant’s GUIDE
P
ractitioner Roster (see “Dementia Diagnosis Attestation” for more information);
• Enrolled in Medicare Parts A and B;
• Not enrolled in Medicare Advantage, including Special Needs Plans (SNPs);
• Have Medicare as their primary payer;
• Not enrolled in the Program of All-Inclusive Care for the Elderly (PACE);
• Has not elected the Medicare hospice benefit; and
• Not a long-term nursing home resident (defined as residence in a nursing home that is not paid
f
or under the Medicare skilled nursing facility benefit)
38
“Community-dwelling” is defined as living in a personal home, assisted living facility, group home, or other
community setting and excludes beneficiaries who become a long-term nursing home resident, defined as a
nursing facility stay that is not covered under the Medicare skilled nursing facility benefit. Beneficiaries will still be
considered community-dwelling for purposes of this model if they are admitted to an acute care hospital or
receive post-acute care in skilled nursing facility.
39
Basic personal everyday activities that include bathing, dressing, transferring, toileting, mobility and eating.
40
Activities related to independent living, including preparing meals, managing money, shopping for groceries or
personal items, performing light or heavy housework, and communication.

19
Beneficiaries who are enrolled in PACE or have elected hospice will not be eligible for alignment to a
G
UIDE Participant because PACE and hospice services could overlap significantly with the services that
will be provided under the GUIDE Model.
Dementia Diagnosis Attestation
Beneficiaries must have dementia to be eligible for alignment to a GUIDE Participant but may be at any
s
tage of dementia—mild, moderate, or severe (note that mild cognitive impairment is not a dementia
diagnosis and is not sufficient to meet this eligibility criteria). To confirm that beneficiaries have
dementia that makes them eligible for the GUIDE Model, CMS will rely on clinician attestation rather
than prior claims-based ICD-10 dementia diagnosis codes.
41
A clinician on the GUIDE Participant’s GUIDE
Practitioner Roster must attest that based on their comprehensive assessment, beneficiaries meet the
National Institute on Aging-Alzheimer’s Association diagnostic guidelines for dementia
42
and/or the
DSM-5 diagnostic guidelines for major neurocognitive disorder.
43
Alternatively, they may attest that
they have received a written report of a documented dementia diagnosis from another Medicare-
enrolled practitioner.
Beneficiary Outreach and Engagement
To maximize the number of beneficiaries who receive services through the GUIDE Model, the GUIDE
Mo
del will use a three-pronged approach to identifying and recruiting potentially eligible beneficiaries:
1) Provider Networks: GUIDE Participants will develop provider networks with primary care
p
roviders, neurologists, hospitalists, hospital discharge planning staff, community-based
organizations, and other relevant groups in the community. Organizations from those networks
may recommend beneficiaries who already have a dementia diagnosis as well as beneficiaries
with suspected dementia but no formal diagnosis to the GUIDE Participant. GUIDE Participants
will work with network organizations to develop appropriate referral criteria and protocols. Any
networks, criteria, and protocols must comply with all applicable fraud and abuse laws.
2) CMS data sharing based on claims: Following a request by the GUIDE Participant, CMS will use
c
laims data from a three-year historical look-back period that falls within the five years prior to
the start date of the Model Performance Period, to identify beneficiaries who received Medicare
services from a GUIDE Participant, have claims-based ICD-10 dementia diagnosis codes, and are
eligible for the GUIDE Model. Using these criteria, CMS will offer GUIDE Participants a one-time
opportunity to request, prior to the GUIDE Participant’s first performance year, a list of eligible
Medicare FFS beneficiaries with dementia diagnosis codes. The list would include beneficiaries
to whom the GUIDE Participant provided services during the three-year historical lookback
41
As discussed in more detail under the section titled Payment Design, after a beneficiary is voluntarily aligned to
the GUIDE Participant, the GUIDE Participant must attach an eligible ICD-10 dementia diagnosis code to each
DCMP claim for the claim to be paid.
42
McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease:
Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic
guidelines for Alzheimer's disease. Alzheimers & Dementia. May 2011; 7(3): 263–269.
43
Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 Approach. Nature
Reviews Neurology. 30 September 2014.

20
period, but who are not currently aligned to the GUIDE Participant. GUIDE Participants will be
able to
use this data to supplement their existing data to reach out to beneficiaries with
dementia who they are serving or have already served. CMS will not automatically align these
beneficiaries to the GUIDE Participant— these beneficiaries must still voluntarily align to the
GUIDE Participant.
3) Beneficiary Outreach Letter: CMS will send targeted outreach letters to eligible beneficiaries
with d
ementia diagnosis codes in their claims’ history, informing them about the GUIDE Model
and how to voluntarily align with a GUIDE Participant in their area, enabling them to self-identify
for the GUIDE Model. Mailings will use sensitive, beneficiary-friendly language and will not
include information about available in-kind beneficiary incentives. This beneficiary identification
pathway is part of the GUIDE Model’s health equity strategy.
To support this outreach, GUIDE Participants will be required to submit to CMS and maintain a
zip-code
based service area encompassing the zip codes from which the GUIDE Participants are
willing to accept beneficiaries. In defining a service area, GUIDE Participants should keep in mind
the GUIDE Model requirements to provide a home visit and GUIDE Respite Services to
beneficiaries in certain model tiers and make referrals to community-based services and
supports. CMS will list multiple GUIDE Participants in the targeted outreach letters if there is
more than one GUIDE Participant in a service area. The beneficiary may decide, in their sole
discretion, which GUIDE Participant to contact if the beneficiary is interested in the GUIDE
Model.
Beneficiary Alignment
After a potentially eligible beneficiary is identified through one of the three pathways described above,
the next s
tep is for the GUIDE Participant to schedule the person with dementia, or suspected dementia,
for an initial comprehensive assessment visit. The GUIDE Participant may choose to do an initial pre-
screening call to rule out beneficiaries who are ineligible for the GUIDE Model, but this is not required.
During the initial comprehensive assessment visit, which is similar to the Medicare service identified by
CPT code 99483, Cognitive Assessment and Planning,
44
the GUIDE Participant’s interdisciplinary care
team will assess the beneficiary and their caregiver (if applicable) across a number of required domains,
including cognitive function, functional status, clinical needs, behavioral and psychosocial needs, and
caregiver burden, with the goal of confirming a dementia diagnosis and creating a comprehensive care
plan.
During the assessment, if the interdisciplinary care team determines that the beneficiary has dementia
and ma
y be eligible to be aligned to the GUIDE Participant, then the care team must obtain the
beneficiary’s consent to voluntarily align to the GUIDE Participant. If the beneficiary, or their legal
representative if applicable,
45
consents, the GUIDE Participant will electronically submit a Patient
44
Cognitive Assessment and Care Plan Services. Centers for Medicare and Medicaid Services.
https://www.cms.gov/cognitive
45
If the GUIDE Participant finds that the beneficiary lacks capacity to consent to voluntarily align to a participant,
the GUIDE Participant will identify and recognize the beneficiary’s legal representative, if any, who has the

21
Assessment and Alignment form to CMS (see Appendix C for a sample Patient Assessment and
Alignment form).
If after the initial assessment, the interdisciplinary care team determines that the beneficiary requires
further testing to confirm a diagnosis, they may refer the beneficiary for such testing. If further testing
confirms a dementia diagnosis, the GUIDE Participant could offer the beneficiary the opportunity to
voluntarily align and submit a Patient Assessment and Alignment form to CMS at that time. If the
interdisciplinary care team assesses a beneficiary, or refers a beneficiary for additional diagnostic
testing, and determines that the beneficiary does not have dementia, the GUIDE Participant can bill for
an appropriate Medicare-covered professional service that corresponds to the service rendered.
The Patient Assessment and Alignment form will include an attestation from a practitioner on the GUIDE
Participant’s GUIDE Practitioner Roster that the beneficiary has dementia. CMS will use the information
submitted on the Patient Assessment and Alignment form to confirm the beneficiary’s eligibility for
alignment to the GUIDE Participant. If CMS finds that the beneficiary is eligible, then CMS will align the
beneficiary to the GUIDE Participant. Figure 1 summarizes the entire beneficiary identification and
voluntary alignment process.
Beneficiary alignment will occur on a rolling, ongoing basis for the first seven years of the GUIDE Model
(July 1, 2024-June 30, 2031). GUIDE Participants will be encouraged to meet a minimum threshold of
200 aligned beneficiaries by the end of their second performance year and maintain this alignment level
throughout the rest of the Model Performance Period.
Beneficiaries will remain aligned to the GUIDE Participant until they become ineligible. For example, an
aligned beneficiary would be deemed ineligible if they no longer meet one of the beneficiary eligibility
requirements or stop receiving model services from the GUIDE Participant (e.g., because they move out
of the program service area, no longer wish to be aligned to the GUIDE Participant, or cannot be
contacted/are lost to follow-up).
To support an organized wind-down of model operations and ensure that all aligned beneficiaries
receive meaningful support from the GUIDE Model, new beneficiaries may not be aligned during the
eighth and final year of the GUIDE Model (July 1, 2031-June 30, 2032).
authority to make health care decisions for the beneficiary (i.e., health care power of attorney, court appointed
legal guardian, etc.), and obtain the legal representative’s consent, acting on behalf of the beneficiary, to
voluntarily align the beneficiary to the GUIDE Participant. The GUIDE Participant will record such legal
representative’s authority to make health care decisions for the beneficiary by keeping a copy of the respective
court order, medical power of attorney, or other relevant document granting the legal representative’s authority
in the beneficiary’s file.

22
Figure 1: New Beneficiary Identification, Eligibility Check, and Voluntary Alignment Process
Model Tiers
CMS will assign aligned beneficiaries to one of five “model tiers,” based on a combination of their
disease stage, whether they have a caregiver, and if applicable, the degree of burden their caregiver is
experiencing. Beneficiary and caregiver complexity, and correspondingly, care intensity and payment,
will increase by tier. See Table 2 for a description of the five tiers.
To ensure consistent beneficiary assignment to tiers across GUIDE Participants, the GUIDE Participant
must use a tool from a set of approved screening tools to measure dementia stage and caregiver
burden. Approved tools have established scoring thresholds that correspond to mild, moderate, and
severe disease stage or caregiver burden. Alternatively, the GUIDE Participant will have the option to
seek CMS approval to use an alternative tool by submitting the proposed tool, along with published
evidence that it is valid and reliable and a crosswalk for how it corresponds to the GUIDE Model’s tiering
thresholds.
The GUIDE Participant receives notification from CMS about whether the
beneficiary is eligible.
Model participant has initial visit with beneficiary and caregiver (if applicable)
and performs comprehensive assessment, including patient history, cognitive
assessment, symptom list, medication history, and caregiver assessment.
CMS uses information submitted on the alignment form to check eligibility in
Medicare systems (e.g., beneficiary is enrolled in Parts A and B, not in hospice)
Identification
Initial
Comprehensive
Assessment Visit
Enrollment Form
to CMS
CMS Eligibility
Check
Beneficiaries are identified in one of three ways:
• Provider referral
• CMS claims-based data sharing with model participants
• Beneficiary self-referral letter sent by CMS
Beneficiaries are identified in one of three ways:
• Provider referral
• CMS claims-based data sharing with model participants
• Beneficiary self-referral letter sent by CMS
Beneficiaries are identified in one of three ways:
• Provider networks
• CMS claims-based data sharing with GUIDE Participant
• Beneficiary outreach letter sent by CMS
Identification
Initial
Comprehensive
Assessment Visit
GUIDE Participant has initial visit with beneficiary and caregiver (if applicable)
and performs comprehensive assessment, including patient history, cognitive
assessment, symptom list, medication history, and caregiver assessment.
At the end of the visit, if the beneficiary consents, the GUIDE Participant
electronically submits a Patient Assessment and Alignment form to CMS
attesting to dementia diagnosis and providing basic beneficiary identifying
information, dementia stage, and caregiver status.
Beneficiary
Alignment Form
to CMS
CMS uses information submitted on the Patient Assessment and Alignment
form to check eligibility in Medicare systems (e.g., beneficiary is enrolled in
Parts A and B, not in hospice, MA, PACE, etc.)
CMS Eligibility
Check
Beneficiary
Alignment

23
The GUIDE Participant will administer the approved screening tools during the initial comprehensive
assessment and submit the resulting scoring data as part of the Patient Assessment and Alignment form.
The GUIDE Participant must additionally electronically submit the individual responses to the caregiver
assessment to CMS.
46
CMS will use this data to assign beneficiaries to a model tier, per the tiering
criteria outlined in Table 2. The GUIDE Participant will be informed of a beneficiary’s model tier
assignment at the same time the GUIDE Participant is informed that a beneficiary is eligible and has
been aligned to them.
The approved measurement tool set will initially include two tools to report dementia stage – the
Clinical Dementia Rating (CDR)
47
and the Functional Assessment Screening Tool (FAST)
48
– and one tool
to report caregiver strain, the Zarit Burden Interview (ZBI).
49
Table 2 shows how these tools correspond
to model tier criteria. For dementia staging tools (the CDR and the FAST), the selected tools include
measures of both cognitive function and activities of daily living (ADL) and/or instrumental activities of
daily living (IADL), as ADL/IADL function is an important determinant of level of need for people with
dementia. Additional tools may be added to the approved measurement tool set throughout the course
of the GUIDE Model. While these are the only specified assessment tools that CMS requires for model
tiering and quality measure development, participants may use other assessment tools necessary to
meet the care delivery requirements.
Table 2: Five Model Tiers and Assignment Criteria
Tier Criteria Corresponding Assessment
Tool Scores
Beneficiaries
with a
caregiver
Low complexity dyad tier Mild dementia CDR= 1, FAST= 4
Moderate complexity dyad
tier
Moderate or severe dementia
AND
Low to moderate caregiver strain
CDR= 2-3, FAST= 5-7
AND
ZBI= 0-60
High complexity dyad tier Moderate or severe dementia
AND
High caregiver strain
CDR= 2-3, FAST= 5-7
AND
ZBI= 61-88
Beneficiaries
without a
caregiver
Low complexity individual
tier
Mild dementia CDR= 1, FAST= 4
Moderate to high
complexity individual tier
Moderate or severe dementia CDR= 2-3, FAST= 5-7
46
CMS will use the caregiver assessment responses to inform the caregiver burden measure development and the
Model’s evaluation.
47
Morris JC. Clinical Dementia Rating: A Reliable and Valid Diagnostic and Staging Measure for Dementia of the
Alzheimer Type. International Psychogeriatrics. 10 January 2005.
48
Sclan SG and Reisberg B. Functional Assessment Staging (FAST) in Alzheimer’s Disease: Reliability, Validity, and
Ordinality. International Psychogeriatrics. 07 January 2005.
49
Bedard M, Molloy DW, Squire L, et al. The Zarit Burden Interview: A New Short Version and Screening Version.
The Gerontologist. October 2021. 41(5): 652-657.

24
Care Delivery
The GUIDE Model will promote high-quality dementia care by defining and requiring GUIDE Participants
to use a comprehensive, standardized care delivery approach for providing care to aligned beneficiaries
and their caregivers. The GUIDE care delivery approach includes 1) a standardized package of services
that the GUIDE Participant must provide to beneficiaries and their caregivers as relevant to the
beneficiary’s preferences and needs based on the person-centered plan (“GUIDE Care Delivery
Services”), 2) an interdisciplinary care team to deliver these services, and 3) a standardized training
requirement for care navigators who are part of the interdisciplinary care team.
Care Delivery Requirements
CMS will require the GUIDE Participant to provide GUIDE Care Delivery Services to its aligned
beneficiaries, as applicable and appropriate to each individual beneficiary’s needs. Table 3 summarizes
the GUIDE Care Delivery Services under nine domains. See Appendix B for detailed requirements of each
care delivery domain.
Table 3. Summary of Required Care Delivery Activities by Domain
Domain
Required Activities by Domain
Comprehensive
Assessment
• Initial comprehensive assessment that includes clinical, behavioral and
psychosocial, and advance care planning domains, as well as caregiver needs and
capabilities and home visit
• Reassessments for beneficiary and caregiver at least once per year
Care Plan
• Develop a comprehensive person-centered care plan that addresses all
assessment domains and is led by the beneficiary
• If the GUIDE Participant is not a primary care practice, ensure the primary care
provider has access to the beneficiary’s person-centered care plan
24/7 Access
• Beneficiary has 24/7 access to an interdisciplinary care team member or help line
(may be a 3
rd
party vendor during off-duty hours)
• Help line must be available to receive ad hoc one-on-one support calls from the
caregiver
Ongoing Monitoring and
Support
• Care navigator is primary point of contact
• GUIDE Participant maintains a minimum contact frequency with the beneficiary
and/or their caregiver. Minimum contact requirements vary by model tier, as
follows:
- Beneficiaries with a caregiver
o
o
o
Low complexity dyad tier: at least quarterly
Moderate complexity dyad tier: at least once a month
High complexity dyad tier: at least once a month
- Beneficiaries without a caregiver
o
o
Low complexity individual tier: at least once a month
Moderate to high complexity individual tier: at least twice a month
Care Coordination and
Transitional Care
Management
• If the GUIDE Participant is not a primary care practice, the GUIDE Participant
must coordinate with the beneficiary’s primary care provider
• Refer beneficiary to specialists to address co-occurring conditions, as needed
• Ensure receipt of information back from specialist to add to care plan
• Support the beneficiary in transitions between personal home and care settings

25
Referral and
Coordination of Services
and Supports
• Maintain or have access to inventory of local/community services
• Refer and connect beneficiaries to community-based services and supports
50
• For dually eligible beneficiaries, coordinate the delivery of any community-based
services and supports with beneficiary’s Medicaid HCBS/LTSS case manager, if
applicable
Medication
Management and
Reconciliation
• Clinician with prescribing authority must review beneficiary’s medications
• Any resulting medication changes must be shared and confirmed with the
beneficiary’s PCP and other relevant specialists
Caregiver Education and
Support
51
• Administer a caregiver support program, which must include:
- caregiver skills training - dementia diagnosis information
- support group services - ad hoc one-on-one support calls
• GUIDE Participant must provide dementia diagnosis information and ad hoc
support calls directly, but may contract with a vendor or a community-based
organization to provide caregiver skills training and/or refer caregivers to
external support group services
Respite
• Referral and coordination of in-home respite care
• Option to refer to adult day centers or facility-based respite providers
The GUIDE Care Delivery Services are the minimum services that the GUIDE Participant is required to
offer beneficiaries. The GUIDE Participant must be able to provide the GUIDE Care Delivery Services at
varying levels of intensity depending on model tier and the beneficiary’s individual needs. The GUIDE
Participant may offer certain additional services outside of the GUIDE Care Delivery Services, including
the in-kind beneficiary engagement incentive permitting GUIDE Participants to use their own funds to
provide environmental modifications to the beneficiary’s home. See section titled, “Authority to Test
the Model”, for more information regarding this beneficiary engagement incentive.
As highlighted in Table 3, the delivery of services will be guided by the creation and maintenance of a
person-centered care plan, which will detail 1) the beneficiary’s goals, strengths, preferences and needs,
2) the results from the comprehensive assessment, 3) recommendations for service providers and
community-based services and supports, including which individual or program is responsible for
payment of each service provider, and 4) the caregiver’s options and preferences for education and
support services (if there is a caregiver). The care plan will also identify the beneficiary’s primary care
provider and any specialists and outline the care coordination services and specialists that are needed to
manage the beneficiary’s dementia and co-occurring conditions.
The requirements also recognize the critical role that caregivers play in caring for people with dementia
by offering caregiver education and support services, as well as including the caregiver, with the
50
For purposes of the GUIDE Model, the term “community-based services and supports” is defined as services and
supports delivered to individuals living in their personal home, assisted living facility, group home, or other
community setting that create or maintain the individual’s ability to safely live in the community. For example, this
term includes, but is not limited to, such services and supports as transportation, home-delivered meals or
groceries, environmental modifications, in home care/assistance, and exercise and socialization activities.
51
Based on our conversations with stakeholders, we anticipate that most beneficiaries will identify a caregiver.
Nevertheless, beneficiaries without caregivers may still receive services under the model. Under such
circumstances, the domains of Caregiver Assessment and Caregiver Education and Support will not apply to that
beneficiary, as a caregiver is not involved to receive those services. Instead, the GUIDE Participant must make
additional efforts and put safeguards into its care delivery services to support beneficiaries without a caregiver.
26
beneficiary’s consent, or the consent of the beneficiary’s legal representative if applicable, in discussions
a
bout the beneficiary’s diagnosis, care, and needs. The GUIDE Participant must administer a caregiver
support program that is based on the caregiver’s needs as identified through the comprehensive
assessment and is responsive to ongoing changes in need. The minimum level of services available to
the caregiver should include caregiver skills training, dementia diagnosis information, and support
services. For support services, at a minimum, the GUIDE Participant must include ad hoc one-on-one
support calls with a member of the care team and referral to support group services.
Care Team Requirements
The GUIDE Participant must maintain an interdisciplinary care team to meet the care delivery
requirements of the GUIDE Model.
At a minimum, the interdisciplinary care team must include a “care navigator” and a clinician with
“
dementia proficiency” who is eligible to bill Medicare Part B evaluation and management services
(E/M), such as a physician, nurse practitioner, physician assistant, or clinical nurse specialist. The
interdisciplinary care team may also include additional members, such as a pharmacist or behavioral
health specialist, at the GUIDE Participant’s discretion.
Care Navigator: To serve as a care navigator under the GUIDE Model, an individual must satisfy the
t
raining requirements described under the section titled “Care Navigator Training.” CMS is not requiring
individuals to have specific professional backgrounds or certifications to work as a Care Navigator,
though CMS believes that registered nurses, licensed clinical social workers, and community health
workers would all be well-suited to this role. The care navigator must be an individual and not artificial
intelligence.
Clinician with dementia proficiency: A clinician will qualify as having “dementia proficiency” if they can
m
eet at least one of the following criteria:
i. Attest to having at least 25 percent of their patient panel (regardless of payer) at some
t
ime in the past 5 years comprised of adults with any cognitive impairment, including
dementia; or
ii. Attest to having at least 25 percent of their patient panel (regardless of payer) at some
time in the past 5 years comprised of adults aged 65 years old or older; or
iii. Have a specialty designation of neurology, psychiatry, geriatrics, geriatric psychiatry,
b
ehavioral neurology, or geriatric neurology.
To be eligible for the established program track, an applicant must attest that their care team includes a
c
linician that meets “dementia proficiency” qualifications when they apply to participate in the GUIDE
Model. Participants in the new program track must complete this attestation when they submit their
Proposed GUIDE Practitioner Roster before the start of their first performance year. If the clinician with
dementia proficiency is not a physician, the GUIDE Participant must have an additional part-time
medical director who is a physician oversee the quality of care for its dementia care program.

27
Care Navigator Training
A comprehensive training program is necessary to support the individuals in the care navigator role,
pa
rticularly since this role can be filled by a non-practitioner lay person such as a community health
worker.
52
The purpose of the training is to provide a foundation for care navigators prior to delivering
services to beneficiaries. The GUIDE Participant must deliver this one-time training when a care
navigator joins the care team, regardless of the care navigator’s professional background.
53
This
required training will also promote consistency of the model intervention by ensuring that care
navigators are receiving training on a standardized set of topics across all GUIDE Participants.
The GUIDE Participant must develop and administer care navigator training that covers certain required
to
pics, as outlined below and described in the Participation Agreement. To the extent possible, the
GUIDE Participant may use a combination of training programs that are already available to meet this
requirement.
An applicant with an established dementia care program may already provide staff trainings that are
largely consistent with the proposed training topics, but they may need to modify, or add to, their
training program to comply with model requirements. GUIDE Participants in the new program track
must develop a training program to comply with model requirements by the start of their first
performance year.
CMS will support GUIDE Participants in both the established program track and the new program track
in
obtaining training and support resources through webinars, affinity groups and written materials. The
GUIDE Model will also provide an online platform for GUIDE Participants to engage with each other to
discuss forums, conferences, and other additional learning opportunities.
The GUIDE Participant’s care navigator training curriculum must address the following topics:
Table 4. Required Care Navigator Training Topics
Topic
Further detail of topic
Background on
Dementia
Overview of dementia as a medical condition; Progression of disease and balancing
dementia with other co-morbidities
Overview of
Assessments
Assessments available related to dementia; Recommendations for a successful
assessment
Care Plan
What is a care plan; Including beneficiary in the development of plan
Person-Centered
Planning
What person-centered planning means; How to incorporate into planning
Challenging Behaviors
Behavioral symptom management; Common behavioral changes due to dementia
and how to address
52
For an overview of the benefits that community health worker programs can bring to health care organizations
and the people they serve, see On the Front Lines of Health Equity: Community Health Workers. U.S. Department
of Health and Human Services. April 2021. https://www.cms.gov/files/document/community-health-worker.pdf
.
53
If an established dementia care program has staff that took training on a model’s required topic in the past five
years and has continued to work for the program during this time, the staff will not need to retake the training on
that topic for the purposes of the model.

28
Functional Needs
What are activities of daily living (ADLs) and instrumental activities of daily living
(IADLs); Evaluation of ADLs and IADLs; Common changes in ADLs and IADLs due to
dementia and how to address; Medication monitoring and maintaining a medication
schedule
Advanced Care Planning
What is an advance medical directive and POLST form; How to assist beneficiary in
advance care planning
Decision-Making
Capacity
What is capacity for medical decision-making; What it means when a beneficiary
does not have capacity for medical decision-making; supported decision-making
Safety
Considerations for safety at home, in public, and driving; elder abuse, neglect, and
financial exploitation; access to weapons and dangerous substances
Communication
Communication strategies for persons with dementia and their caregivers
Coordination of medical
care and community
services
Communication with clinical providers; Supporting beneficiary in transitions
between settings; Accessing community-based services and supports, including
respite services; Working with case managers and other coordinators to address
gaps and duplication in a beneficiary’s community-based services and supports
Supporting a Caregiver
Caregiver strain and support (e.g.: peer-to-peer support, support group, 1:1
support); In-home caregiver training and importance of caregiver education
Diversity in Dementia
Treating dementia and communicating with diverse populations in a culturally
competent way
The training must be a minimum of 20 hours, including a minimum of 10 hours of didactic instruction
plus a minimum of 10 hours of experiential training, e.g., job shadowing of experienced care navigators,
supervised interactions with beneficiaries, case studies, or on-the-job training. The minimum of 10 hours
of didactic instruction may be live or a web-based training. The minimum of 10 hours of experiential
training must be live, not asynchronous. The GUIDE Participant must develop an assessment for care
navigators to take after the training to ensure comprehension.
Care navigators must take an additional 2 hours of training each year. This training may be developed
an
d offered by the GUIDE Participant or be a continuing education training offered by a third party.
Care Delivery Reporting
The GUIDE Participant will complete care delivery reporting at least once per year, which will consist of a
se
ries of questions about how they are implementing the care delivery requirements of the GUIDE
Model, including how frequently they are interacting with aligned beneficiaries and their caregivers and
what care modalities they are using. Care delivery reporting will also include a Health Equity Plan
section, as discussed in the “Health Equity Strategy” section.
GUIDE Participants in the established program track will be required to complete their first care delivery
re
porting during a 60-day window that will begin one month before the start of the Model Performance
Period (June 1, 2024—July 31, 2024). This “baseline” care delivery reporting will enable CMS to
understand GUIDE Participants’ capabilities at the beginning of the GUIDE Model and assess how they
evolve over time. Beginning in their second performance year, established program track participants
will complete care delivery reporting, including health equity plan submission, annually at the start of
each performance year.
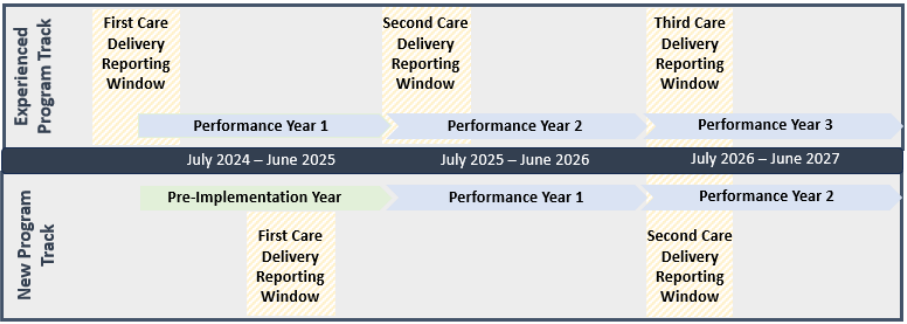
29
GUIDE Participants in the new program track will be required to complete their first care delivery
reporting by May 1, 2025, which is two months before the beginning of their first performance year. This
reporting will be used to determine whether new program track participants are able to meet the care
delivery requirements of the GUIDE Model before starting their first performance year. Beginning in
their second performance year, new program track participants will be required to complete care
delivery reporting, including health equity plan submission, on the same timeline as established
participants (i.e., annually at the start of each performance year).
Figure 2: Care Delivery Reporting Timeline
Performance Measurement
CMS will adjust GUIDE Participants’ monthly DCMP based on the GUIDE Participant’s performance on a
set of performance metrics that align with the GUIDE Model’s goals, so that GUIDE Participants are
financially rewarded when they achieve these goals for their aligned beneficiaries and held accountable
when they do not.
Performance Metrics
To the extent possible, the CMS Innovation Center aims to minimize provider burden and create
alignment across CMS by selecting performance measures for the GUIDE Model that are already being
used in other CMS programs. In particular, the CMS Innovation Center aims to align to the extent
feasible with the MIPS Value Pathway (MVP) called “Supportive Care for Neurodegenerative Conditions
MVP” (“Neuro MVP”), which focuses on the clinical theme of promoting high quality care for patients
with cognitive-based neurological disorders, including but not limited to dementia.
CMS will also develop two new metrics to assess GUIDE Participant performance: a measure of caregiver
burden and a metric of long-term nursing home utilization.
CMS intends to eventually include five measures in the GUIDE performance measure set: one clinical
quality process measure, two patient-reported outcome measures, one cost measure, and one
utilization measure. Table 5 provides an overview of the five measures and is followed by a more
detailed discussion of each measure. The five measures in the performance measure set will be used to
adjust GUIDE Participants’ monthly payments. CMS plans to phase in the use of these measures over

30
time. See the “Performance-Based Adjustment” section for details on how this adjustment will be
calculated.
Table 5: GUIDE Performance Measure Set
Measure Name Aligned Model Goals MIPS, NQF
Measure?
Neuro
MVP?
Measure Type &
Mode
Use of High-Risk Medications in
Older Adults
Improve beneficiary quality
of life; reduce hospital and
ED utilization
MIPS: Yes, #238
NQF: Yes, #0022
Yes Process
CQM
eCQM
Quality of Life Outcome for
People with Neurological
Conditions
Improve beneficiary quality
of life
MIPS: Yes,
#AAN22
NQF: No
Yes PROM
Survey (Registry)
Caregiver Burden Measure Reduce caregiver burden MIPS: No
NQF: No
No PROM
Survey
Total Per Capita Cost (TPCC) Reduce cost of care MIPS: Yes
NQF: Yes, #3575
No Cost
Claims-based
New: Rate of beneficiaries
entering a long-term nursing
home stay
Prevent or delay long-term
nursing home stays; reduce
cost of care (or maintain
budget neutrality)
MIPS: No
NQF: No
No Utilization
Claims-based
Use of high-risk medications in older adults (MIPS #238, NQF #0022)
54
: Medication-related issues,
including prescription of contraindicated medications and non-adherence to recommended
medications, are common among people with dementia and can lead to avoidable hospitalizations and
ED use.
55,56
This process measure assesses the percentage of patients 65 years of age and older who
were ordered two or more high-risk medications. This measure is part of the Neuro MVP.
Quality of life outcome for people with neurological conditions (MIPS #AAN22): Beneficiary quality of
life will be the primary patient-reported outcome measure (PROM) for the GUIDE Model. This PROM
measures the percentage of patients whose quality-of-life assessment results are maintained or
improved during the measurement period, and is reported through a registry. This measure is part of
the Neuro MVP.
Caregiver Burden Measure: Reducing caregiver burden is another primary model objective, for which
there is not an existing outcomes measure. CMS will develop a measure of this purpose and use a
54
Link to the Neuro MVP measure specifications: https://qpp.cms.gov/mips/explore-mips-value-pathways/M0004
55
El-Saifi N, Moyle W, Jones C, and Tuffaha H. Medication Adherence in Older Patients with Dementia: A
Systematic Literature Review. Journal of Pharmacy Practice. May 2017. 31(3).
56
Wucherer D, Thyrian JR, Eichler T et al. Drug-related problems in community-dwelling primary care patients
screened positive for dementia. International Psychogeriatrics. August 2017.

31
survey-based tool to capture the burden and strain caregivers encounter in their caregiving role. The
measu
re development process could take several years.
Total per capita cost (TPCC) (NQF #3575): The TPCC measure will measure performance on costs and
incen
tivize reductions in a variety of avoidable utilization categories, including hospital, ED, and post-
acute care. TPCC is a MIPS measure.
Rate of beneficiaries entering a long-term nursing home: A metric of long-term nursing home stays is
impor
tant because nursing home delay or avoidance is expected to be a key source of model savings.
There is no existing performance measure that fully captures long-term nursing home stays in older
adults (existing measures are specified for Medicaid managed care, and either include primarily short-
term nursing home stays or are more appropriate for adults with intellectual and developmental
disabilities).
57
Rather than fully develop a new, validated performance measure, CMS will calculate a
performance rate and benchmarks using CMS administrative data, which will allow CMS to incorporate
this metric into the performance-based payment adjustment more quickly (i.e., in the first or second
model performance year). Specifically, CMS will use the CMS Minimum Data Set file to identify
beneficiaries residing in a nursing home whose stay is not covered under the Medicare skilled nursing
facility benefit.
Performance Benchmarks
CMS will compare GUIDE Participants’ scores on the five model performance metrics to performance
bench
marks in order to determine their performance-based adjustment (see “Payment Design” section
for more information on the PBA). CMS will calculate performance benchmarks that are specific to the
GUIDE Model (in other words, CMS will not use benchmarks from other programs, such as MIPS). Where
possible, when measures are claims-based, CMS will calculate benchmarks from a blend of both GUIDE
Participants and non-participants.
For non-claims-based measures, where non-participant data is unavailable, CMS will calculate
bench
marks from GUIDE Participant data alone. For such measures, in later years of the GUIDE Model,
CMS may consider modifying benchmarks as more data becomes available.
To ensure that CMS is setting accurate and meaningful benchmarks for GUIDE Participants, the GUIDE
Model wil
l have a “pay for reporting” approach for the first year of the Model Performance Period for
the non-claims-based measures (beneficiary quality of life and high-risk medication utilization). Viewing
the distribution of data from this year will allow CMS to set appropriate performance benchmarks for
future years. Based on the data reported in the first year of the Model Performance Period, CMS will set
benchmarks for each measure and keep them constant for the second and third years. For example, for
the quality-of-life measure, GUIDE Participants in the established program track will receive credit for
reporting quality data for July 1, 2024 – June 30, 2025. CMS will use this data to calculate performance
benchmarks. These benchmarks will be used to assess performance for GUIDE Participants in both the
new and established program tracks in the second and third years of the Model Performance Period.
After the third year, based on the two additional years of quality data, CMS will decide whether to
57
CMS SMD# 22-003 RE: Home and Community-Based Services Quality Measure Set:
https://www.medicaid.gov/federal-policy-guidance/downloads/smd22003.pdf

32
continue to hold the benchmarks constant or update the benchmark for future years. Participants in the
new program track will not have pay for reporting, since their first performance year will be the second
year of the Model Performance Period, when benchmarks have been established.
For the claims-based measures (TPCC and Long-Term Nursing Home Stay Rate), benchmarks for the first
year of the Model Performance Period will be calculated based on claims data from prior to the Model
(e.g., CY 2022). Benchmarks will then be updated for the second year based on data from the first year.
Benchmarks will be kept constant for the third year, after which time CMS will decide whether to update
the benchmarks.
On an annual basis, CMS will publish a methodology paper with the technical specifications and
benchmarks for the performance measures. The methodology paper will be made available to GUIDE
Participants 30 days before the applicable performance year.
Table 6: GUIDE Performance Metric Benchmarks
Measure Benchmark group Timing
Use of High-Risk Medications
in Older Adults
GUIDE Participants -Pay for reporting PY 1
-PY 2 and PY 3 benchmark based on PY 1 data
-CMS to decide how to update benchmarks
after PY 3 and publish information in the
annual methodology paper
Quality of Life Outcome for
People with Neurological
Conditions
GUIDE Participants -Pay for reporting Year 1
-PY 2 and PY 3 benchmark based on PY 1 data
-CMS to decide how to update benchmarks
after PY 3 and publish information in the
annual methodology paper
Caregiver Burden Measure GUIDE Participants Pending measure development process
Total Per Capita Cost GUIDE Participants and non-
participants within a
geographic region
-Based on CY 2023 data for PY 1
-PY 2 and PY 3 benchmark based on PY 1 data
-CMS to decide how to update benchmarks
after PY 3 and publish information in the
annual methodology paper
Rate of beneficiaries with a
long-term nursing home stay
GUIDE Participants and non-
participants
-Based on CY 2023 data for PY 1
-PY 2 and PY 3 benchmark based on PY 1 data
-CMS to decide how to update benchmarks
after PY 3 and publish information in the
annual methodology paper
Payment Design
The GUIDE Model will include a monthly per beneficiary care management payment: the Dementia Care
Management Payment (DCMP). CMS will adjust the DCMP for health equity and performance on a set of
performance measures. The GUIDE Model will also include two other payments: a payment for GUIDE
Respite Services and a one-time infrastructure payment for safety net providers in the new program
track (if eligible).

33
The five main components of the GUIDE Model’s payment methodology are:
1) Monthly DCMP (tiered by patient complexity);
2) A health equity adjustment to the DCMP;
3) A performance-based payment adjustment to the DCMP;
4) A payment for GUIDE Respite Services; and
5) A one-time infrastructure payment for safety net providers in the new program track (if eligible)
Dementia Care Management Payment
The DCMP is designed to offer GUIDE Participants more flexibility to deliver personalized dementia care
th
an is possible under traditional FFS. It will cover a more comprehensive set of services than existing
care management codes, be less burdensome to bill, and allow for payment to members of the
interdisciplinary care team who are otherwise not eligible to bill for Medicare services. The DCMP also
will not be subject to beneficiary cost sharing. GUIDE Participants will continue to bill for all services not
included in the DCMP under traditional FFS.
GUIDE Participants will use a set of new G-Codes created for the GUIDE Model to submit claims for the
mo
nthly DCMP. The DCMP is intended to cover the GUIDE Care Delivery Services (with the exception of
GUIDE Respite Services, which is paid for under a separate respite payment).
Each model tier will have a different DCMP rate to reflect the fact that covered services and care
in
tensity will vary across the tiers. For example, for tiers that include beneficiaries without a caregiver,
the DCMP does not incorporate payment for caregiver education and support. However, the DCMP
rates also reflect the fact that beneficiaries without a caregiver are expected to have more intensive
care needs than beneficiaries at a similar disease stage who have a caregiver.
The DCMP rate will also be higher for the first six months that a beneficiary is aligned to a GUIDE
Part
icipant to reflect the high intensity of initial program activities, such as the comprehensive
assessment, home visit, and establishment and implementation of a new care plan. Beginning in the
seventh month after the beneficiary is aligned to a GUIDE Participant, the DCMP rate for that beneficiary
will be lower. Each model tier will have two G-codes, for a total of 10 DCMP G-codes: a “new patient”
code for the first six months that a beneficiary is aligned to the GUIDE Participant and an “established
patient” code for after the first six months. Table 7 shows the DCMP G-code base rates, by model tier
and length of alignment.
The GUIDE Participant will be responsible for billing the correct G-code for each aligned beneficiary each
mo
nth, based on the beneficiary’s model tier and length of alignment. The GUIDE Participant must
attach an eligible ICD-10 dementia diagnosis code to each DCMP claim for it to be paid; DCMP claims
without an eligible ICD-10 diagnosis code will be denied.
58
In order to support accurate billing, CMS will
provide each GUIDE Participant with a monthly beneficiary alignment file that lists all the beneficiaries
58
Initial list of eligible ICD-10 dementia diagnosis codes will include: F01.50, F01.511, F01.518, F02.80, F02.811,
F02.818, F03.90, F03.911, F03.918, G30.0, G30.1, G30.8, G30.9, G31.1, G31.2, G31.01, G31.09, G31.83. Eligible
code list may change over time to reflect updates to ICD-10 codes.

34
aligned to that GUIDE Participant, their model tier assignment, and the length of their alignment to the
GUIDE Participant.
Table 7: Per Beneficiary Per Month (PBPM) Base Payment Rates
Beneficiaries with
Caregiver: Low
Complexity Dyad
Tier
Beneficiaries with
Caregiver:
Moderate
Complexity Dyad
Tier
Beneficiaries with
Caregiver: High
Complexity Dyad
Tier
Beneficiaries
without
Caregiver: Low
Complexity
Individual Tier
Beneficiaries
without Caregiver:
Moderate to High
Complexity
Individual Tier
First 6 months
(New Patient
Payment Rate)
$150 $275 $360 $230 $390
After first 6 months
(Established Patient
Payment Rate)
$65 $120 $220 $120 $215
The DCMP rates above represent base payment rates and will be adjusted for geographic variation in
costs as well as cost growth over time.
To account for geographic variation in costs, CMS will adjust the DCMP base rates by the Medicare
Geographic Adjustment Factor (GAF) for each DCMP claim submitted by a GUIDE Participant. The GAF
applied to the DCMP is a weighted geographic adjustment based on all services in the Medicare PFS. It
summarizes the combined impact of the 3 Geographic Practice Cost Index (GPCI) expense categories
(work, practice expense, malpractice) on a locality’s (state or metropolitan region’s) physician
reimbursement level.
59
To account for cost growth over time, CMS will annually update the DCMP base rates by the Medicare
Economic Index (MEI)
60
, a measure of physician practice cost growth calculated by the CMS Office of the
Actuary.
Movement between tiers
The GUIDE Participant will be required to re-assess aligned beneficiaries on at least an annual basis. The
GUIDE Participant will have the discretion to re-assess beneficiaries more frequently; however, CMS will
only accept aligned beneficiary re-assessments from a GUIDE Participant once every 180 days for
purposes of the beneficiary moving between tiers. Based on the results of the re-assessment, CMS could
assign aligned beneficiaries to either a higher or lower tier, leading to either an increase or decrease in
payment rates. When an aligned beneficiary is re-assessed into a new tier, in the following month the
GUIDE Participant will be eligible to bill the G-code for the established patient payment rate associated
with that tier. The GUIDE Participant will submit re-assessment results to CMS using the Patient
Assessment and Alignment Form (see Appendix C).
Cost-sharing for the DCMP
59
Updated GAF amounts are published annually as part of the Medicare Physician Fee Schedule regulation
addenda: https://www.cms.gov/medicare/medicare-fee-for-service-payment/physicianfeesched/pfs-federal-
regulation-notices
60
For further information on MEI calculations visit https://www.cms.gov/newsroom/fact-sheets/effect-medicare-
economic-index-mei-physician-update

35
The DCMP amount will cover both face-to-face and non-face-to-face services in one lump sum. Cost
sharing for non-face-to-face services like chronic care management codes has historically been a
significant barrier to utilization of these services. CMS will waive the standard 20% coinsurance for the
DCMP and CMS will pay the GUIDE Participant 100% of the appropriate DCMP rate rather than 80% for
purposes of the GUIDE Model.
Additional Guidance on billing duplicative FFS codes
The DCMP will replace fee-for-service payment for some existing Medicare Physician Fee Schedule (PFS)
services, including chronic care management and principal care management, transitional care
management, advance care planning, and technology-based check-ins. Therefore, the GUIDE Participant
will not be able to bill separately for these services for aligned beneficiaries. CMS will provide GUIDE
Participants, who are participating in multiple CMS Innovation Center models, with additional
instruction related to billing these services (see section titled, “Program Overlaps and Synergies”). Table
8 provides the set of services that GUIDE Participants will not be able to bill for aligned beneficiaries.
CMS may add or remove codes from this list over time to reflect changes in Physician Fee Schedule
billing codes.
Table 8: Medicare Physician Fee Schedule Services Included Under DCMP
Service Type
HCPCS Codes
Advance care planning
99497, 99498
Welcome to Medicare and Annual Wellness Visits
G0402, G0438, G0439
Home Health Care Plan Oversight
G0181
Hospice Care Plan Oversight
G0182
Cognitive Assessment and Planning
99483
Technology-based check-in services
G2012, G2252
Transitional Care Management
99495-99496
Chronic Care Management
99487, 99489-99491, 99437, 99439, G0506
Principal Care Management
99424–99427
Administration of patient-focused health risk assessment (HRA)
96160
Administration of caregiver-focused HRA
96161
Depression screening
G0444
Group Caregiver Behavior Management/ Modification Training
Services* 96202, 96203
Caregiver Training Services under a Therapy Plan of Care
established by a PT, OT, SLP* 97550, 97551, and 97552
Community Health Integration Services*
G0019, G0022
Principal Illness Navigation Services*
G0023, G0024, G0140, and G0146
Administration of a Standardized, Evidence-based Social
Determinants of Health Risk Assessment* G0136

36
* Services listed on the 2024 Physician Fee Schedule proposed rule which will become effective on or
after January 1, 2024.
Health Equity Adjustment
The GUIDE Health Equity Adjustment (HEA) is designed to provide additional resources to GUIDE
Participants to deliver care to beneficiaries from underserved communities. CMS will calculate an HEA
for each beneficiary that is aligned to a GUIDE Participant, based on the beneficiary’s health equity
score. The HEA will be calculated annually, and then applied to the DCMP for each beneficiary as a
monthly adjustment. The HEA is intended to be budget neutral to minimize the financial impact on the
overall model.
The HEA will be calculated using a composite methodology that includes both area-level and beneficiary-
level measures of deprivation. Specifically, the HEA will be composed of four measures: state and
national comparison Area Deprivation Index (ADI), which are measured at the census block group
61
level, and Low-Income Subsidy (LIS) status and dual eligibility (DE), which are beneficiary-level measures.
CMS will calculate an Equity Score for every beneficiary b and their corresponding geography g in the
aligned population:
In the above formula, National ADI
g
is the ADI national percentile of the census block group the
beneficiary resided in on their first day of eligibility and can range from 1 to 100. State ADI
s
is the ADI
state decile of the census block group the beneficiary resided in on their first day of eligibility, and can
range from 1 to 10, corresponding to the state decile. CMS is using LIS and DE as the beneficiary-level
variables. CMS is including both measures even though CMS expects significant overlap between these
two measures because the objective of this policy is to increase access regardless of a beneficiary’s full
or partial dual status. LIS
b
represents LIS status and is equal to 1 if the beneficiary receives the LIS, and
0 otherwise. Similarly, DE
b
represents dual eligibility and is equal to 1 if the beneficiary is dually eligible
and 0 otherwise. The possible range of health equity scores is from 0 to 40. In the case of a maximum
score, a beneficiary’s National ADI would contribute 25%, State ADI would contribute 25%, and LIS or DE
status would contribute 50% to the overall score. The equity score formula weights are designed to help
CMS most accurately identify underserved populations. The contribution of each factor to the final score
balances geographic deprivation in low-income states, geographic deprivation in high-income states,
and individual-level income status. LIS/DE is weighted more generously than the area-level measures to
ensure that beneficiary-level measures are meaningfully contributing to the beneficiary’s overall equity
score. CMS may revisit this weighting based on the geographic makeup of participants.
CMS will calculate beneficiary health equity scores and percentiles annually, before the start of the
performance year in which they are applied. Because beneficiaries will not be aligned to GUIDE
Participants at the time of model launch, the first health equity adjustments will not be applied to the
DCMP until the start of the second year of the Model Performance Period, and will be determined based
61
Census block groups are the next level above census blocks in the geographic hierarchy that is used by the U.S.
Census Bureau to report aggregated census data. A census block group is a combination of census blocks.

37
on data from the first year of the Model Performance Period. Beneficiary health equity scores and
percentiles will be reassessed each subsequent year. Table 9 shows how health equity scores are
translated into an adjustment to the monthly DCMP.
Table 9. Equity Score Percentiles and Associated Health Equity Adjustment Amounts
Equity Score Percentile Health Equity Adjustment to DCMP
≥80
th
percentile of equity scores +$15
51
st
-79
th
percentile of equity scores $0
0-50
th
percentile of equity scores -$6
This adjustment methodology is designed to provide a material incentive for GUIDE Participants to care
for underserved beneficiaries and to be budget neutral while limiting the magnitude of any downward
adjustments. CMS may elect to add other measures to the GUIDE Model’s HEA in future performance
years.
Performance-Based Adjustment
The performance-based adjustment (PBA) will increase or decrease GUIDE Participants’ monthly DCMPs,
depending on how they performed on the GUIDE Model’s five performance metrics during the previous
performance year (see the “Performance Measurement” section for more information on the
performance metrics and benchmarks). The PBA will be applied as an ongoing percentage adjustment to
each GUIDE Participant’s monthly DCMP. Once all the performance metrics are fully phased in, GUIDE
Participants can increase their DCMP amount by up to 10% through high performance or decrease their
DCMP by as much as -3.5% for poor performance.
Timing of PBA
The GUIDE Participant’s performance during a given performance year will affect their payment in
future years. Specifically, the GUIDE Participant’s performance will be calculated beginning three
months after the end of the performance year to allow time for reporting and claims run-out, and the
resulting PBA will be applied to the GUIDE Participant’s DCMP beginning six months after the end of the
performance year, and continuing for 12 months. In other words, there is a six-month lag between the
end of the performance year and when results begin to affect payment. For example, for the established
program track, the first performance year will be July 2024 through June 2025 and the resulting PBA will
be applied from January 2026 through December 2026. Figure 3 demonstrates this timeline. The new
program track will follow the same timeline but beginning one year later and with one less performance
year.
Figure 3: Timing of Performance Year and Corresponding Performance-Based Adjustment

38
Calendar Year 2025 2026 2027 2028 2029 2030 2031 2032
Established
Program
Track
PY 1
7/2024 –
6/2025
PY 2
7/2025 –
6/2026
PY 3
7/2026 –
6/2027
PY 4
7/2027 –
6/2028
PY 5
7/2028 –
6/2029
PY 6
7/2029 –
6/2030
PY 7
7/2030 –
6/2031
PY 8
7/2031 –
6/2032
PBA 1
1/2026-
12/2026
PBA 2
1/2027-
12/2027
PBA 3
1/2028-
12/2028
PBA 4
1/2029-
12/2029
PBA 5
1/2030-
12/2030
PBA 6
1/2031-
12/2031
PBA 7
1/2032-
06/2032
New
Program
Track
Pre-
Implement-
ation Year
PY 1
7/2025 –
6/2026
PY 2
7/2026 –
6/2027
PY 3
7/2027 –
6/2028
PY 4
7/2028 –
6/2029
PY 5
7/2029 –
6/2030
PY 6
7/2030 –
6/2031
PY 7
7/2031 –
6/2032
PBA 1
1/2027-
12/2027
PBA 2
1/2028-
12/2028
PBA 3
1/2029-
12/2029
PBA 4
1/2030-
12/2030
PBA 5
1/2031-
12/2031
PBA 6
1/2032-
06/2032
PBA Domains, Measures, and Weights
Each of the GUIDE Model’s five performance measures will be assigned to one of four domains: care
coordination and management, beneficiary quality of life, caregiver support, and utilization.
Each domain, and each measure within a domain, is associated with a minimum and maximum potential
PBA amount that GUIDE Participants can earn. How much of the potential PBA amount GUIDE
Participants earn for a given measure is determined by their performance. The amount that GUIDE
Participants earn for each measure will then be added together to determine their total PBA.
As discussed in more detail below, scoring works differently for domains with a single measure versus
domains with multiple measures. There will also be a distinct scoring approach for the two pay-for-
reporting measures in the first year of the Model Performance Period.
Scoring for domains with a single measure
For the three domains with a single measure (care coordination and management, beneficiary quality of
life, and caregiver support), there will be four performance categories – fail, no adjustment, pass, and
exceed. The performance thresholds and associated percentage payment adjustments are as follows:
Table 10: Measure Performance Categories and Associated Payment Adjustments for Domains with a
Single Measure
Performance Category Percentage Adjustment Earned
Fail -1%
No adjustment 0%
Pass 1.5%
Exceed 3%
Note: Please see the “Performance Measurement” section for more information on how CMS will set the
performance benchmarks that determine the cut-off points between each category.
Scoring for the utilization domain
39
CMS will establish pass/fail benchmarks for the measures in the utilization domain. As shown in Table
11, for each measure in the utilization domain, the GUIDE Participant will receive 1.5% positive
adjustment for a pass or a 0.5% negative adjustment for a fail, for a maximum of possible score in the
overall domain of a three percent positive adjustment (+3%) or a one percent negative adjustment (-
1%).
Table 11: Measure Performance Categories and Associated Payment Adjustments for Utilization
Domain
Performance Category Percentage Adjustment Earned
Fail -0.5%
Pass 1.5%
Scoring for Pay-for-Reporting in First Year of the GUIDE Model
As discussed in the “Performance Measurement” Section, in the first year of the Model Performance
Period, CMS will use a pay-for-reporting methodology for the two non-claims-based measures—high-
risk medication utilization and beneficiary quality of life. This means that GUIDE Participants in the
established program track will receive full credit for reporting measure data, regardless of their
performance. For the high-risk medication measure, the maximum PBA potential for reporting will be
+1%. For the quality-of-life measure, the maximum PBA potential for reporting will be +2%. GUIDE
Participants will receive a 0% adjustment for any measure they fail to report.
Table 12: Pay-for-Reporting Payment Adjustments
Performance Measure Percentage Adjustment Earned
for Reporting
Percentage Adjustment Earned
for Non-Reporting
High-risk medication utilization +1%
0%
Beneficiary quality of life +2%
0%
Summary of PBA Domains, Measures, and Associated PBA Potential

40
Table 13 summarizes how the measures will be assigned to domains and an associated PBA potential
once all of the quality metrics are fully phased in.
Table 13: PBA Domains, Measures, and Weights in later Model Performance Years, Once All
Performance Measures are Phased In
Domain Domain
Weight
Measure Name Percent of
total domain
Percent of
total PBA
Associated PBA
Potential
Care coordination
and management
10% Use of High-Risk
Medications in Older
Adults
100% 10% -.5% – +1%
Beneficiary
quality of life
30% Quality of Life Outcome
for People with
Neurological Conditions
100% 30% -1% – +3%
Caregiver support 30% New: Caregiver Burden
Measure
100% 30% -1% – +3%
Utilization 30% Total Per Capita Cost 50% 15% -.5% – +1.5%
Rate of beneficiaries
entering a long-term
nursing home
50% 15% -.5% – +1.5%
Total PBA Potential -3.5% to +10%
As a result of measure phase-ins and the development time for certain measures, we anticipate that the
maximum PBA adjustment will be no more than 6% and no lower than -1% in the first year of the Model
Performance Period, and no more than 7% and no lower than -2.5% in the second year of the Model
Performance Period. Tables 14 and 15 show how domain weights will differ in the first two years of the
GUIDE Model.
Table 14: PBA Domains, Measures, and Weights for First Year of the GUIDE Model
Domain Domain
Weight
Measure Name Percent of
total domain
Percent of
total PBA
Associated PBA
Potential
Care
coordination
and
management
16% Use of High-Risk
Medications in Older
Adults
100% 16% 0% - +1%
Beneficiary
quality of life
34% Quality of Life Outcome
for People with
Neurological Conditions
100% 34% 0% - +2%
Utilization 50% Total Per Capita Cost 50% 25% -.5% – +1.5%
Rate of beneficiaries with
a long-term nursing home
stay
50% 25% -.5% – +1.5%
Total PBA Potential -1% to +6%

41
Table 15: PBA Domains, Measures, and Weights for Second Year of the GUIDE Model (e.g., PY 2 for the
established program track and PY 1 for the new program track)
Domain Domain
Weight
Measure Name Percent of
total domain
Percent of
total PBA
Associated PBA
Potential
Care
coordination
and
management
14% Use of High-Risk
Medications in Older
Adults
100% 20% -.5% – +1%
Beneficiary
quality of life
43% Quality of Life Outcome
for People with
Neurological Conditions
100% 40% -1% – +3%
Utilization 43% Total Per Capita Cost 50% 21.5% -.5% – +1.5%
Rate of beneficiaries with
a long-term nursing home
stay
50% 21.5% -.5% – +1.5%
Total PBA Potential -2.5% to +7%
Example PBA Calculations
Example #1:
In the first year of the GUIDE Model, one measure will be under development, and two measures will be
pay-for-reporting. Table 16 shows an example PBA calculation for the first year of the GUIDE Model.
Table 16: Example PBA calculation for established program in first year of the GUIDE Model
Domain Measure Performance Achieved PBA
Care Coordination and
Management
High-risk medications Data reported (Pass) +1%
Beneficiary quality of life Quality of life outcome Data reported (Pass) +2%
Caregiver Support Caregiver Burden Measure
(in development)
n/a n/a
Utilization TPCC measure Fail -0.5%
Long-term nursing home stay
rate
Pass +1.5%
Total PBA Earned +4%

42
Example #2:
Table 17 shows an example PBA calculation for a GUIDE Participant once all performance measures are
fu
lly phased in.
Table 17: Example PBA calculation once all performance measures are fully phased in
Domain
Measure
Performance Achieved
PBA
Care Coordination and
Management
High-risk medications
Pass
+1%
Beneficiary quality of life
Quality of life outcome
Exceed
+3%
Caregiver Support
Caregiver Burden Measure
Exceed
+3%
Utilization
TPCC measure
Pass
+1.5%
Long-term nursing home stay rate
Pass
+1.5%
Total PBA Earned
+10%
Respite Payment
GUIDE Participants must provide, or contract with another organization to provide, in-home GUIDE
Res
pite Services to aligned beneficiaries who are eligible to receive GUIDE Respite Services
62
(see
below, Eligibility Requirements for Aligned Beneficiaries to Receive GUIDE Respite Services). GUIDE
Participants may also choose to provide, or contract with another organization to provide, GUIDE
Respite Services provided in an adult day center
63
or a facility that can provide 24-hour care. The GUIDE
Participant has the flexibility to use a combination of any or all of these respite options for each
beneficiary eligible to receive GUIDE Respite Services.
The GUIDE Participant will bill for GUIDE Respite Services by submitting claims using three new respite
G-co
des created for the GUIDE Model, one for each setting of care (in-home, adult day, and facility-
based). Respite payments will not be made on a claim-by-claim basis; instead, CMS will aggregate the
respite payments and make one monthly respite payment for all GUIDE Respite Services billed in the
preceding month.
The in-home respite G-code will cover a 4-hour unit of service and be paid at $104; the adult day respite
G-c
ode will cover an 8-hour unit paid at $78; the facility-based respite G-code will cover a 24-hour unit
paid at $260. The GUIDE Participant can bill as many or as few of the codes as needed for an eligible
beneficiary, up to a per beneficiary annual cap of $2,500.
64
In order to help the GUIDE Participant track
62
GUIDE Respite Services are temporary services provided to a beneficiary in their home, at an adult day center, or
at a facility that can provide 24-hour care, for the purpose of giving the caregiver a break from caring for the
beneficiary.
63
Adult day center, as used herein, refers to adult day care, adult medical day care, adult day services, adult day
health centers, and other commonly used terms that describe centers that provide care for older adults similar to
the entities listed here.
64
The GUIDE respite allotment of $2,500 per year equates to roughly 96 hours of in-home GUIDE Respite Services
per year, paid at a rate of $26 per hour. If the GUIDE respite allotment were used solely at an adult day center, it

43
how close beneficiaries are to the annual cap, CMS will provide the GUIDE Participant with a monthly
payment file showing the amount of GUIDE Respite Services that each aligned beneficiary has used in
the year to-date.
The respite G-codes and the annual respite cap will be geographically adjusted using the same
methodology as the DCMP; they will be updated annually by the amount of the Home Health Agency
market basket less the productivity adjustment (a metric that is calculated by the CMS Office of the
Actuary for the Home Health Prospective Payment System to measure cost growth for home health
agencies).
65
The respite payment will not have beneficiary cost sharing and will be paid at 100% of the
determined amounts.
The GUIDE Participant must bill for all GUIDE Respite Services rendered to aligned beneficiaries. If the
GUIDE Participant provides GUIDE Respite Services by contracting with another organization, the GUIDE
Participant is responsible for entering into a contract with the organization, billing for the GUIDE Respite
Services, and then reimbursing the organization.
As detailed in paragraph 6.2 of the GUIDE Care Delivery Services, for dually eligible beneficiaries who
receive respite care through a state Medicaid program, the GUIDE Participant shall contact and attempt
to coordinate the delivery of GUIDE Respite Services with the beneficiary’s Medicaid state agency
and/or Medicaid managed care plan’s case manager. GUIDE Respite Services are intended to be additive
to, and not duplicative of, any available Medicaid respite care benefit offered to dually eligible
beneficiaries. The GUIDE Participant is prohibited from billing under both the GUIDE Model and
Medicaid for the same unit of respite (e.g., billing under both the GUIDE Model and Medicaid for the
same 24-hour nursing home stay).
Eligibility Requirements for Aligned Beneficiaries to Receive GUIDE Respite Services
An aligned beneficiary must meet the following requirements in order to be eligible to receive GUIDE
Respite Services:
i. have a caregiver; and
ii. be assigned to either the moderate complexity dyad tier or the high complexity dyad tier.
Requirements for Respite Providers to Provide GUIDE Respite Services
As discussed under the section titled “Program Integrity Screening”, CMS will conduct a program
integrity screening of all applicants and their proposed Partner Organizations, which includes any
Medicare-enrolled and non-Medicare enrolled respite providers, as part of the application review
process. CMS will confirm that the GUIDE Participant, or the contracted organization furnishing GUIDE
Respite Services, complies with the qualifications to provide GUIDE Respite Services under the GUIDE
Model.
would cover 32 days of adult day per year; if it were used solely for facility-based care, it would cover roughly 10
days of facility-based care per year.
65
Additional information regarding the Home Health Agency market basket and productivity adjustment can be
found at: https://www.cms.gov/research-stat
istics-data-and-systems/statistics-trends-and-
reports/medicareprogramratesstats/marketbasketdata.
44
The GUIDE Participant must also ensure that they, or the contracted organization furnishing GUIDE
Respite Services, complies with the qualifications to provide GUIDE Respite Services under the GUIDE
Model, and that any direct care workers that provide in-home GUIDE Respite Services meet the
requirements listed below, at all times that the GUIDE Participant, or organization, is providing GUIDE
Respite Services.
In order to qualify to provide GUIDE Respite Services under the GUIDE Model, in-home respite
providers, adult day centers, and facilities that can provide 24-hour care must be one of the following:
i. a Medicare-certified facility that can provide 24-hour care or a Medicare-certified provider
that provides in-home respite services;
ii. a Medicaid-certified adult day center, Medicaid-certified facility that can provide 24-hour
care, or a Medicaid-certified provider that provides in-home respite services; or
iii. a company or organization licensed or certified with the state, in which they are providing
services, to provide one of the following services:
a. respite,
b. home care,
c. residential services,
d. adult day services, or
e. residential facility or group home (not a private residence).
In addition, any direct care workers that provide in-home GUIDE Respite Services must:
i. be at least 18 years old,
ii. have passed a background check,
iii. be licensed or certified as a direct care worker in the state in which they are providing
services if such licensure or certification is a requirement to work as direct care worker in
the state, and
iv. meet the training requirements to be a direct care worker, if any, of the state in which they
are providing services.
If the GUIDE Participant, or the contracted organization furnishing GUIDE Respite Services, loses their
Medicare certification, Medicaid certification, state license or state certification, they will no longer be
permitted to provide GUIDE Respite Services. The GUIDE Model will not pay, and GUIDE Participants
may not bill, for GUIDE Respite Services provided by a GUIDE Participant, or a contracted organization
furnishing GUIDE Respite Services, that loses their Medicare certification, Medicaid certification, state
license or state certification.
Example GUIDE Respite Services Claim:
The following is an example claim for GUIDE Respite Services calculated over one month. This example is
illustrative in nature and intended to give applicants a baseline understanding of how the respite
payments will be calculated.
Beneficiary B has a caregiver and is in the severe model tier. This claim is for one month’s worth of
GUIDE Respite Services.

45
In Home Care: 4-Hour unit 16 hours (4 units) $104 $416
Adult Day Center: 8-Hour Unit 8 hours (1 unit) $ 78 $ 78
Facility: 24-Hour Unit 48 hours (2 units) $ 260 $ 520
Total GUIDE Respite Services
$ 1,014
*The GAF is also calculated for the respite payments but do not count towards the total annual cap.
To calculate the amount of the GUIDE respite payment available for the GUIDE Participant to furnish the
GUIDE Respite Services under the GUIDE Model for rest of the year: $2500 - $1014 = $1486
Payment Examples
The first two payment examples below show how total GUIDE Model payments will be calculated for an
individual aligned beneficiary over the course of a full performance year. The third example shows how
total GUIDE Model payments will be calculated for a GUIDE Participant’s total aligned beneficiary
population. The examples assume that all beneficiaries are newly aligned in the first month of the
performance year, and therefore are eligible for the new patient DCMP rate for the first six months of
the year and the established patient DCMP rate for the next six months. All examples are assumed to
occur after the PBA and HEA are fully phased in but reflect the current base rate and do not account for
future MEI updates. In the first example, the beneficiary is in a tier that is eligible for GUIDE Respite
Services, and the example assumes that she reaches the respite cap for the year. In the second example,
the beneficiary is in a tier that is not eligible for GUIDE Respite Services. The third example assumes that
all beneficiaries eligible for GUIDE Respite Services reach their respite cap for the year. Examples are
rounded to the nearest dollar.

46
Payment Example #1: Beneficiary in the Moderate Complexity Tier with Caregiver
Payment Example #2: Beneficiary in the Moderate/Severe Complexity Tier without Caregiver
Note: Example 3 is a stylized example and does not include the HEA, which is a beneficiary level
adjustment. The HEA could increase or decrease participants’ total payment. It also assumes that all
patients are aligned at the beginning of the year as new patients.
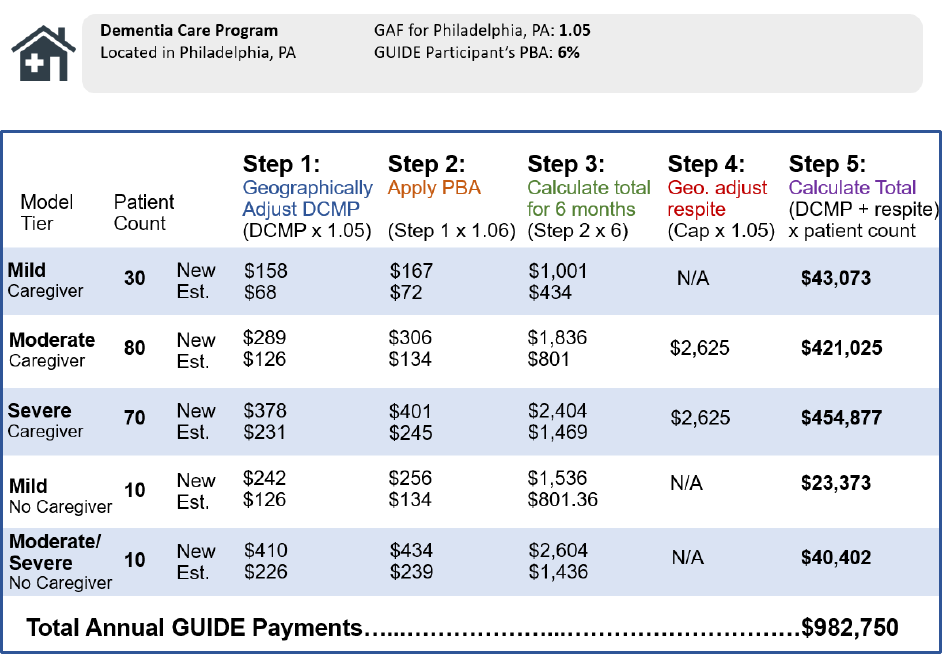
47
Payment Example #3: Dementia Care Program
Infrastructure Payment
In addition to technical assistance and support, GUIDE Participants in the new program track that are
classified as safety net providers will be eligible to receive an infrastructure payment to cover some of
the upfront costs of establishing a new dementia care program. This payment is intended for GUIDE
Participants who want to develop new dementia care programs to serve underserved beneficiaries but
need upfront resources to get started. The infrastructure payment will be a one-time payment of
$75,000 made at the beginning of the pre-implementation period. The payment will be geographically
adjusted using the same PFS GAF that will be used to adjust the DCMP.
The infrastructure payment is intended to assist GUIDE Participants in the new program track that
qualify as safety net providers with: 1) hiring, 2) training, 3) developing program workflows, protocols,
community partnerships, and materials, 4) community outreach and engagement, and 5) electronic
health record technology adaptations. Infrastructure payment funds may only be used for costs in these
five categories. GUIDE Participants will be required to report on how they used infrastructure funds as
part of their care delivery reporting.
GUIDE Participants will be required to pay the infrastructure payment back to CMS if they withdraw or
are terminated from the GUIDE Model. GUIDE Participants that withdraw or are terminated before the
start of the second performance year will be required to repay the whole infrastructure payment to

48
CMS. GUIDE Participants that withdraw from the GUIDE Model or are terminated during the second
performance year will be required to repay half of the infrastructure payment.
Safety net provider eligibility determination
To qualify as a GUIDE safety net provider, a new program applicant must have a Medicare FFS
beneficiary population comprised of at least 36% beneficiaries receiving the Part D low-income subsidy
(LIS) or 33.7% of beneficiaries who are dually eligible for Medicare and Medicaid. These thresholds are
based on the safety net definition that the Innovation Center has developed to assess and track safety
net provider participation in its models.
66
CMS will use Medicare claims to assess the composition of an
applicant’s Medicare FFS beneficiary population and determine whether they meet the safety net
criteria. CMS will notify the selected applicant of whether they meet the GUIDE safety net criteria before
the deadline to sign their Participation Agreement.
If an applicant plans to create a new TIN for the purposes of participating in the GUIDE Model, then in
order to be assessed for the GUIDE safety net provider criteria, at time of application, the applicant must
provide to CMS a Proposed GUIDE Practitioner Roster that is as similar as possible to the Proposed
GUIDE Practitioner Roster that the applicant will submit two months prior to their first Performance
Year (see section titled, “Participation Requirements” for more information on application requirements
for GUIDE Participants in the new program track) if accepted to participate in the Model. The Proposed
GUIDE Practitioner Roster must include at least one clinician with dementia proficiency and list the
historical TIN(s) under which each practitioner(s) on their Proposed GUIDE Practitioner Roster has
previously billed for Part B services.
At the time of the GUIDE safety net provider eligibility determination, CMS will deem a beneficiary to be
part of an applicant’s beneficiary population in the following order of precedence:
1) If the beneficiary selected, on Medicare.gov, one of the Medicare-enrolled physicians or non-
physician practitioners listed on the applicant’s Proposed GUIDE Practitioner Roster;
2) If the applicant or one or more practitioners from the applicant’s Proposed GUIDE Practitioner
Roster furnished the plurality of the beneficiary’s qualifying CPT/HCPCS code services (see Table
18 for a list of CPT or HCPCS Codes Used to Identify Applicant’s Beneficiary Population) over the
past two years; or
3) If the applicant or one or more practitioners from the applicant’s Proposed GUIDE Practitioner
Roster billed the beneficiary’s most recent claim (if that claim was for an Annual Wellness Visit
or a Welcome to Medicare Visit) during the most recently available 24-month period.
At the time of determination, CMS will also confirm whether each applicable beneficiary:
1) Received a qualifying service from the GUIDE Participant (defined at the TIN level – please see
paragraph above on the GUIDE Model’s policy for applicants who create a new TIN for purposes
of participating in the GUIDE Model) during the lookback period (see Table 18 below);
66
Person-Centered Innovation–An Update on the Implementation of the CMS Innovation Center’s Strategy–
Supplemental Document. November 7, 2022. https://innovation.cms.gov/media/document/cmmi-strategy-imp-
update-tech

49
2) Has both Medicare Parts A and B;
3) Has Medicare as their primary payer; and
4) Was not enrolled in a Medicare Advantage plan.
The following list of patient encounter codes will be used to identify an applicant’s beneficiary
population according to the process outlined above for purposes of the GUIDE safety net provider
determination:
Table 18. HCPCS Codes Used to Identify Applicant’s Beneficiary Population
Service
Code
Office/Outpatient Visit E/M
99201-99205, 99211-99215, G2212
Nursing Facility, FQHC, and RHC Services
99304-99310; 99315, 99316- 99318
Complex Chronic Care Coordination Services
99487
Chronic Care Management (CCM) Services
99489-99491, 99437, 99439, G2058
Principal Care Management (PCM)
99424-99427, G2064, G2065
Transitional Care Management Services
99495-99496
Home Care/Domiciliary Care E/M
99324-99328, 99334-99337, 99339-99345,
99347-99350
Online Digital E/M
99421-99423
Audio-Only Telephone E/M
99441-99443, G2252
Technology-based check-in services
G2010, G2012, G2252
Advance Care Planning
99497, 99498
Depression, substance use disorder, and alcohol
misuse screening and counseling services
G0396-G0397, G0442-G0444
Welcome to Medicare and Annual Wellness Visits
G0402, G0438, G0439
Assessment/care planning for patients requiring
CCM services
G0506
Care management services for behavioral health
conditions
99484
Cognition and functional assessment for patient
with cognitive impairment
99483
Administration of patient-focused health risk
assessment (HRA)
96160
Administration of caregiver-focused HRA
96161
Psychiatric Collaborative Care Model
99492-99494, G0511, G0512, G2214
Outpaent clinic visit for assessment and
management (for crical
access hospital-based outpaent primary care
pracces)
G0463

50
Health Equity Strategy
The Innovation Center believes that equitable care is a key component of achieving high-quality care for
beneficiaries and is therefore critical to the GUIDE Model’s success. CMS defines health equity as: “the
attainment of the highest level of health for all people, where everyone has a fair and just opportunity
to attain their optimal health regardless of race, ethnicity, disability, sexual orientation, gender identity,
socioeconomic status, geography, preferred language, or other factors that affect access to care and
health outcomes.”
67
The term “underserved communities” refers to populations sharing a particular
characteristic, as well as geographic communities, that have been systematically denied a full
opportunity to participate in aspects of economic, social, and civic life.
68
Along with the health equity adjustment to model payments, the new program track and infrastructure
payment for safety net providers, the Referral and Coordination of Services and Supports domain in care
delivery, and the requirement for care navigator training to include a cultural competency domain, the
GUIDE Model has two additional model requirements which are designed to promote health equity:
1) Health Equity Plan Requirement
2) Health Equity Data Collection Requirement
Health Equity Plan Requirement
GUIDE Participants will be required to develop and implement a Health Equity Plan. The purpose of a
Health Equity Plan is for each GUIDE Participant to identify disparities in outcomes in their patient
populations and implement initiatives to measure and reduce these disparities over the course of the
GUIDE Model.
On an annual basis, GUIDE Participants will be required to report on the progress of their Health Equity
Plan as a section of the GUIDE Model’s care delivery reporting. The focus of health equity planning will
be on improving quality of care for underserved beneficiaries and addressing health disparities. GUIDE
Participants will be required to set goals and monitor progress over time, identifying and selecting
evidence-based interventions for addressing health disparities and achieving equitable outcomes. The
Innovation Center will provide a framework for Health Equity Plans, and will review, but not assess,
plans submitted by GUIDE Participants.
The first Health Equity Plan will be due as part of the baseline care delivery reporting (see “Care
Delivery” section for more information about reporting timeline). The first Health Equity Plan must focus
specifically on beneficiary outreach and engagement as a precursor to more comprehensive annual
Health Equity Plans. The goal of the first Health Equity Plan will be to encourage GUIDE Participants to
67
CMS Framework for Health Equity 2022-2023. Centers for Medicare and Medicaid Services. April 2022.
https://www.cms.gov/files/document/cms-framework-health-equity-2022.pdf
68
Executive Order on Advancing Racial Equity and Support for Underserved Communities Through the Federal
Government. January 20, 2021. https://www.whitehouse.gov/briefing-room/presidential-
actions/2021/01/20/executive-order-advancing-racial-equity-and-support-for-underserved-communities-through-
the-federal-government/

51
develop and implement strategies to reach potentially eligible beneficiaries from historically
underserved communities from the outset of the GUIDE Model.
GUIDE Participants will be required to prepare and submit comprehensive Health Equity Plans beginning
in the second care delivery reporting period, at the start of GUIDE Participants’ second performance
year, and update the plans annually thereafter.
Health Equity Plans may not propose or use actions that selectively target beneficiaries based on race,
ethnicity, national origin, disability, religion, or sex. In addition, Health Equity Plans must comply with all
applicable non-discrimination laws, including section 1557 of the Affordable Care Act, Title IX of the
Education Amendments of 1972, Title VI of the Civil Rights Act of 1964, and Section 504 of the
Rehabilitation Act. GUIDE Participants will be permitted to identify beneficiaries for health equity plan
interventions based on other factors, including but not limited to medical history, health status, health
needs, disability status, or income, provided the GUIDE Participant and other individuals or entities
performing functions or services related to the Health Equity Plan comply with all applicable non-
discrimination laws and regulations.
Health Equity Data Collection Requirement
CMS will require all GUIDE Participants to collect and report certain beneficiary-reported
sociodemographic data and health-related social needs (HRSN) data from their aligned beneficiaries
willing to share this information. To avoid discouraging beneficiaries from accessing care from GUIDE
Participants, beneficiaries are not required to share this data with their providers. GUIDE Participants
are not required to report this data to CMS for any beneficiary who chooses not to disclose them.
HRSNs are used to describe individual-level social needs and are individual-level, adverse social
conditions that negatively impact a person’s health or health care.
Some GUIDE Participants may
already be collecting HRSNs from their beneficiaries, but it is important that all GUIDE Participants
collect this information to provide adequate services, plan for future interventions, and increase quality
of care. HRSN collection and referrals will be part of the GUIDE Model’s broader care delivery
requirements for comprehensive assessment and referral for social services and supports.
GUIDE Participants will be encouraged to use one of two preferred HRSN screening tools: the
Accountable Health Communities (AHC) HRSN Screening tool
70
or the Protocol for Responding to and
Assessing Patient’s Assets, Risks, and Experiences (PRAPARE) tool.™
,
71
GUIDE Participants will be
required to annually report HRSN data that is aggregated across aligned beneficiaries and includes
domains such as: food insecurity, housing instability, transportation needs, utility difficulty, and
interpersonal safety. This data collection will allow CMS and GUIDE Participants to evaluate health
inequities and disparities in GUIDE communities.
70
The Accountable Health Communities Health-Related Social Needs Screening Tool. Center for Medicare and
Medicaid Innovation. https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf
71
PRAPARE Screening Tool. https://prapare.org/the-prapare-screening-tool/
52
GUIDE Participants will also be required to collect and report a core set of sociodemographic measures
o
n an annual basis from their aligned beneficiaries willing to share this information. The data elements
in this core set will use standardized United States Core Date for Interoperability (USCDI) definitions.
Example measures are race, ethnicity, sex assigned at birth, disability status, and preferred language.
Learning Systems Strategy
The GUIDE learning system will include: 1) a learning community for all GUIDE Participants, and 2) virtual
coaching and facilitation provided by CMS for GUIDE Participants in the new program track.
The GUIDE Participant Learning Community will:
• Facilitate the provision of technical assistance, reaching GUIDE Participants with written
m
aterials and communication about the GUIDE Model payment, requirements, deadlines, and
conditions for participation.
• Capture, document, and disseminate tactics and strategies in the provision of comprehensive
d
ementia care.
• Foster peer-to-peer sharing of tools, experience, and tactics.
• Provide opportunities for GUIDE Participants to convene and share experiences and resources
regionally or nationally, through existing in-person meetings or new virtual meetings.
• Provide opportunities for learning and peer-to-peer sharing of strategies for improving health
e
quity.
Coaching and facilitation for GUIDE Participants in the new program track will use a virtual group
c
oaching approach. CMS will offer coaching sessions in group settings to allow GUIDE Participants to
learn from each other’s experiences and include brief didactics (how-tos) and case-based learning with
cases presented by GUIDE Participants to expert faculty on challenges, questions, etc. that arise as they
establish their dementia care programs. Topics for the coaching sessions could include developing a
caregiver support program or a care navigator training program. Coaching sessions will occur during the
pre-implementation period and the first performance year for the new program track.
Data
Data Reporting Requirements
In accordance with 42 CFR 403.1110(b), any entity participating in the testing of an Innovation Center
m
odel is required to collect and report such information, including “protected health information” as
defined in 45 CFR 160.103, as the Secretary determines is necessary to monitor and evaluate the GUIDE
Model. Below is a list of all data elements that the GUIDE Participant will be required to report to CMS.
• Beneficiary and Caregiver Assessment Data (See Beneficiary Eligibility and Beneficiary Alignment
section)
• Quality Data (See Performance Measurement section)
• Care Delivery Reporting (See Care Delivery section)
• Sociodemographic Data (See Health Equity Data Collection Requirement section)
53
• Health-related social needs (See Health Equity Data Collection Requirement section)
Data Sharing
Data sharing is an important tool for helping GUIDE Participants understand how they are doing relative
to other GUIDE Participants, track their performance over time, identify trends, and target areas for
improvement. GUIDE Participants will be strongly encouraged to use data sharing provided under the
GUIDE Model to i) assess their model implementation; ii) measure effects on quality of care; and iii)
develop data-based strategies to improve both model implementation and quality of care. The model
learning system will support GUIDE Participants in understanding how to use their data for quality
improvement efforts. Under the GUIDE Model, there will be two primary sources of data sharing:
1) Data Dashboard: The primary platform that CMS will use to share data with GUIDE Participants
is through the GUIDE Data Dashboard. The Data Dashboard will provide GUIDE Participants with
an interactive, user-friendly interface for viewing claims-based utilization data for their aligned
beneficiaries, updated monthly. Data will be available and aggregated across the GUIDE
Participant’s entire aligned population, for domains including hospitalizations, physician
services, and post-acute care. The Data Dashboard will also incorporate quality and
sociodemographic data reported by GUIDE Participants, so that they can view key data points
within a single tool. The Data Dashboard will also show GUIDE Participants how they compare to
peer organizations on important quality and utilization outcomes.
2) Monthly payment and beneficiary alignment files: On a monthly basis, CMS will provide GUIDE
Participants with a beneficiary alignment and payment file. The beneficiary alignment file will
show which beneficiaries are aligned to the GUIDE Participant, their model tier assignment, and
other beneficiary-level data. The payment file will provide data on GUIDE payment amounts for
each aligned beneficiary and aggregated across the GUIDE Participant’s total aligned beneficiary
population.
The data sharing and data analytics in the GUIDE Model will comply with all applicable laws, including
the privacy and security requirements promulgated under the Health Insurance Portability and
Accountability Act of 1996 (HIPAA). GUIDE Participants will be required to submit a HIPAA-Covered Data
Disclosure Request and Attestation (DRA) form to request the specific types of data that the GUIDE
Participants will need to perform certain health care operations activities related to the GUIDE Model
and will attest that the data requested is the minimum necessary to perform those activities, consistent
with HIPAA rules and regulations. CMS will provide the DRA to be completed by the Participant.
All GUIDE Participants will be required to provide beneficiaries and their caregivers with information
about how to modify their data sharing preferences and opt out of claims data sharing of beneficiary-
identifiable information for care coordination and quality improvement purposes.
In the event the Innovation Center develops new, center-wide data sharing strategies, including data
aggregation, during the Model Performance Period, CMS will also strive to align GUIDE data sharing with

54
these strategies as appropriate. CMS will also consider publicly reporting performance data as part of
our Innovation Center model data sharing initiative.
72
Participant Monitoring, Auditing, and Termination Strategy
CMS will monitor GUIDE Participants on a regular, ongoing basis. CMS will use GUIDE Participant care
delivery reporting, beneficiary and caregiver assessment data, GUIDE Practitioner Rosters, Partner
Organization Rosters, claims, cost, utilization, and quality data in its monitoring strategy.
Regular program monitoring may result in audits of select GUIDE Participants. Data that GUIDE
Participants submit to CMS, performance on utilization and quality measures, referral and billing
patterns, and other practice information may trigger an audit of GUIDE Participants with anomalous
findings. CMS may also randomly select GUIDE Participants for audit.
GUIDE Participants will be informed of the possibility of being selected for an audit and will be required
to maintain copies of all documentation related to their use of model payments and their
implementation of the GUIDE Model in case of an audit. More information related to the GUIDE Model’s
record retention policy will be provided in the Participation Agreement.
CMS reserves the right to terminate a GUIDE Participant’s Participation Agreement at any time during
the term of the Participation Agreement for reasons associated with poor performance, program
integrity issues, non-compliance with the terms and conditions of the Participation Agreement, or as
otherwise specified in the Participation Agreement or required by section 1115A(b)(3)(B) of the Social
Security Act.
Evaluation
All GUIDE Participants will be required to cooperate with CMS efforts to conduct an independent,
federally-funded evaluation of the GUIDE Model, which may include completion of surveys and
participation in interviews, site visits, and other activities that CMS determines necessary to conduct a
comprehensive evaluation. The evaluation will use a mixed-methods approach to assess both model
impact and implementation experience.
Authority to Test the Model
Authority to Test the Model
The GUIDE Model will be operated under Section 1115A of the Social Security Act (the Act) (added by
Section 3021 of the Affordable Care Act) (42 U.S.C. 1315a). Section 1115A of the Act establishes the
Innovation Center for the purpose of testing innovative payment and service delivery models to reduce
Medicare and Medicaid expenditures while preserving or enhancing the quality of care furnished to
beneficiaries of such programs.
Section 1115A(b)(2) of the Act requires the Secretary “to select models to be tested from models where
the Secretary determines that there is evidence that the model addresses a defined population for
72
CMMI Model Data Sharing Model Participation Data Initiative. Center for Medicare and Medicaid Innovation.
https://resdac.org/cms-data/files/cmmi-model-data-sharing-cmds-model-participation-data-initiative
55
which there are deficits in care leading to poor clinical outcomes or potentially avoidable expenditures.”
The GUIDE Model addresses a defined population (community-dwelling, Medicare FFS beneficiaries,
including beneficiaries dually eligible for Medicare and Medicaid, who have dementia) for which there
are deficits in care resulting in both poor outcomes and potentially avoidable expenditures in
unnecessary hospital, emergency department (ED), and post-acute care utilization.
Waiver and OIG Safe Harbor Authority
Under section 1115A(d)(1) of the Act, the Secretary of Health and Human Services may waive such
requirements of Titles XI and XVIII and of sections 1902(a)(1), 1902(a)(13), 1903(m)(2)(A)(iii), and certain
provisions of section 1934 of the Act as may be necessary solely for purposes of carrying out section
1115A with respect to testing models described in section 1115A(b).
For this model and consistent with the authority under section 1115A(d)(1), the Secretary may consider
issuing waivers of certain fraud and abuse provisions in sections 1128A, 1128B, and 1877 of the Act. No
fraud or abuse waivers are being issued in this document; fraud and abuse waivers, if any, would be set
forth in separately issued documentation. Any such waiver would apply solely to the GUIDE Model and
could differ in scope or design from waivers granted for other programs or models. Thus,
notwithstanding any provision of this RFA, GUIDE Participants must comply with all applicable laws and
regulations, except as explicitly provided in any such separately documented waiver issued pursuant to
section 1115A(d)(1) specifically for the GUIDE Model.
In addition to or in lieu of a waiver of certain fraud and abuse provisions in sections 1128A and 1128B of
the Act, CMS may determine that the anti-kickback statute safe harbor for CMS-sponsored model
arrangements and CMS-sponsored model patient incentives (42 C.F.R. § 1001.952(ii)) is available to
protect remuneration exchanged pursuant to certain financial arrangements or patient incentives
permitted under the GUIDE participation documentation. No such determination is being issued in this
document. Such determination, if any, would be set forth in documentation separately issued by CMS.
Benefit Enhancement and Beneficiary Engagement Incentive
The GUIDE Model will use the authority under section 1115A(d)(1) of the Act to make available the
telehealth benefit enhancement and the environmental modification beneficiary engagement incentive.
Telehealth benefit enhancement
If necessary during the Model Performance Period, CMS intends to make available to GUIDE Participants
a conditional waiver of (1) the “originating site” requirements at section 1834(m)(4)(C) of the Social
Security Act and 42 CFR § 410.78(b)(3)–(4) with respect to telehealth services furnished to eligible
beneficiaries; (2) the “originating site” requirement in the eligible telehealth individual provision at
section 1834(m)(4)(B) of the Social Security Act with respect to telehealth services being “furnished at
an originating site”; and (3) the “originating site” facility fee provision in section 1834(m)(2)(B) of the
Social Security Act and 42 CFR § 414.65(b) with respect to telehealth services furnished to an aligned
beneficiary at their home.
56
Environmental modification beneficiary engagement incentive
CMS also intends to permit GUIDE Participants to use their own funding to provide in-kind
e
nvironmental modifications to the beneficiary’s home of a total value of up to $1,000 per beneficiary
per year. Environmental modifications will contribute to a safer home environment for the beneficiary
and provide the beneficiary with tools to continue to live at home.
The environmental modification shall be either (i) an item purchased by the Participant and delivered to
t
he Beneficiary or (ii) the Participant will arrange and pay for installation of the environmental
modification by a handy worker or home improvement contractor. The environmental modification
must have a reasonable connection to the beneficiary’s health care and not promoted or marketed to
potential beneficiaries. Depending on the beneficiary’s needs, environmental modifications could
include expenses for modifications such as grab bars, flexible shower head, safer flooring, signs, or
improved lighting.
This beneficiary engagement incentive will be optional for GUIDE Participants to make available to
aligned beneficiaries. If the GUIDE Participant offers this beneficiary engagement incentive, it must be
offered in addition to the care delivery requirements detailed in Appendix B and in accordance with the
requirements described in the Participation Agreement. The GUIDE Participant will be required to retain
certain documentation in conjunction with the provision of this in-kind incentive.
Merit-Based Incentive Payment System (MIPS) Alternative Payment Model (APM) and
Advanced APM Status
MIPS APM: An Innovation Center model may be considered a MIPS APM if it meets two criteria: 1)
participants in the Model (“APM Entities”) participate under an agreement with CMS or through a law or
regulation; and 2) the APM bases payment on quality measures and cost/utilization. CMS requires
GUIDE Participants to sign a participation agreement with CMS and bases payment on utilization and
quality measures through the performance-based adjustment. Therefore, the GUIDE Model will satisfy
both MIPS APM criteria and is expected to qualify as a MIPS APM.
Advanced APM: A model (or track within a model) must meet three specific criteria to be considered an
A
dvanced APM: 1) require use of Certified Electronic Health Record Technology (CEHRT), 2) provide for
payment based on performance on MIPS-comparable quality measures, and 3) require participants to
bear a more than nominal amount of financial risk. We do not expect GUIDE to qualify as an Advanced
APM because it does not meet the financial risk standard.
Because we expect the GUIDE Model to be a MIPS APM, we also expect that any MIPS-eligible clinician
w
ho is included on a GUIDE Participant’s GUIDE Practitioner roster will be eligible for voluntary scoring
under the APM Performance Pathway as described at 42 CFR § 414.1367.
Program Overlaps and Synergies
CMS will allow organizations (identified at the TIN level) to participate in both the GUIDE Model and all
other current Innovation Center models for which they meet the eligibility criteria, as well as the
Medicare Shared Savings Program (Shared Savings Program). Individual practitioners (identified at the
57
NPI level) and Partner Organizations will also generally be permitted to be part of a GUIDE Practitioner
R
oster or Partner Organization Roster and furnish services under other current Innovation Center
models and the Shared Savings Program. Current and future Innovation Center models may establish
their own model overlaps policies with the GUIDE Model as well. The following sections discuss overlap
policies for three types of models and programs: Shared Savings Program and Innovation Center ACO
models; BPCI Advanced and Comprehensive Care for Joint Replacement (CJR) Models; and Innovation
Center models that have care management payments.
Overlaps with Shared Savings Program and Innovation Center ACO Models
Participant overlap
CMS will allow participant overlap at the TIN and NPI level with the ACO Realizing Equity, Access, and
C
ommunity Health (REACH) model, the Shared Savings Program, and the three Comprehensive Kidney
Care Contracting (CKCC) Options in the Kidney Care Choices (KCC) Model.
Beneficiary overlap
Eligible beneficiaries may simultaneously be aligned to the GUIDE Model and attributed to participants
i
n ACO REACH, the Shared Savings Program, or the CKCC options in KCC. For beneficiaries who are
aligned to both a GUIDE Participant and a participant in ACO REACH, the Shared Savings Program, or the
CKCC Options of the KCC model, the GUIDE Model will share beneficiary-level data on GUIDE Model
payments with each of these programs, allowing them the flexibility to account for these payments in
their benchmarking or spending calculations.
In 2024, the Innovation Center’s Total Cost of Care Models will not include the DCMP and respite
p
ayments in the shared savings calculations. Beginning in July 2025 or July 2026, the DCMP (including
the performance-based adjustment, health equity adjustment, and the respite payments) made to a
GUIDE Participant for an aligned beneficiary may be included in an ACO’s expenditures and benchmarks.
Beginning July 1, 2024, the DCMP and respite payments made to a GUIDE Participant for an aligned
b
eneficiary will count towards the shared savings/losses in the Medicare Shared Savings Program. In
future years, GUIDE payments may be included in ACO benchmark and expenditure calculations.
Overlaps with the BPCI Advanced and Comprehensive Care for Joint Replacement (CJR) Models
Participant overlap
The GUIDE Model will allow participant overlap with the BPCI Advanced model at the TIN level.
H
owever, given the differing clinical focuses of these models and the GUIDE Model, we would expect
this type of overlap to be rare.
Beneficiary overlap
Eligible beneficiaries may simultaneously be aligned to a GUIDE Participant and a participant in the BPCI
A
dvanced and CJR models. GUIDE Model payments will not be incorporated into BPCI Advanced or CJR
episode reconciliation calculations. CJR overlap will only be relevant for 6 months, as CJR is scheduled to
end in December 2024.
58
Overlaps with Innovation Center models that have care management payments
Participant overlap
The DCMP includes care coordination services similar to other Innovation Center models such as Primary
Care First (PCF), Making Care Primary (MCP), the Maryland Primary Care Program (MDPCP), the
Enhancing Oncology Care Model (EOM), and Kidney Care First (KCF). GUIDE will permit participant
overlap at the TIN and NPI level with PCF, MCP, MDPCP, EOM, and KCF.
Beneficiary overlap
Eligible beneficiaries may simultaneously be aligned to a GUIDE Participant in the GUIDE Model and
attributed or aligned to participants in active CMMI models, including ACO Reach, Kidney Care Choices,
Making Care Primary, Maryland Total Cost of Care Model, Primary Care First, and Vermont All Payer
Model. The same provider or supplier cannot receive payment for care coordination under the GUIDE
Model and another model for treating the same beneficiary who may be aligned or attributed to both
models. If such an overlap occurs, the GUIDE Model will reconcile the overlap amount for that provider
retrospectively. If only the beneficiary, and not the provider, or only the provider and not the
beneficiary, overlaps with two models that have care management payments, then no payment will be
recouped.

59
Appendices
Appendix A: Participant Application Guidance and Questions
This document is not the application to be filled out by the applicant; this is a list of the questions that
may be found in the online application portal and is provided for reference only. The online application
portal can be accessed via a link on the GUIDE Model website: https://innovation.cms.gov/innovation-
models/guide. All GUIDE applications must be submitted through the online application portal by 11:59
pm Eastern Daylight Time on January 30, 2024.
CMS may seek additional information from applicants to the GUIDE Model after the application period
closes. Not all applicants are guaranteed participation in the GUIDE Model. In selecting participants,
CMS will consider factors critical to ensuring a robust evaluation of the GUIDE Model. CMS may also
deny individual clinicians or any other individual or entity participation in the GUIDE Model based on
the results of a program integrity review.
CMS will safeguard the information provided in accordance with the Privacy Act of 1974, as amended (5
U.S.C. § 552a). For more information, please see the CMS Privacy Policy at https://www.cms.gov/
privacy.
For questions regarding the GUIDE Model or the GUIDE application process, email
Complete Profile (Section 1)
Organization Information (Tab 1)
1. GUIDE Model Applicant Information
Legal Business Name:
Doing Business As (DBA):
Organization TIN/EIN:
Street Address:
City:
State:
ZIP Code:
Website, if applicable:
2. How would you define your organization (Check all that apply or check N/A if your
organization is not on this list):
. Physician Group Practice/Clinic
. Health System
. Accountable Care Organization (ACO)
. Hospice Agency
. Home Health Agency (HHA)
. Other Group Practice/Clinic
. N/A
60
3. Did the applicant submit a Letter of Interest (LOI) for the GUIDE Model? (Optional) (A Letter
of Interest is not a requirement to apply for the Model, this information will only be used for
tracking purposes)
. Yes
. No
If yes, please note the number on your LOI submission _______
4. Provide an executive summary describing the applicant including the history/context of
applicant’s interest in the Model, the applicant’s strategies and goals for forming a
dementia care program, and the applicant’s fit with the Model’s goals. [5000 character
limit]
5. Explain how participation in the GUIDE Model will allow your organization to deliver
comprehensive dementia care to the populations you serve. Include how your participation
in the GUIDE Model will expand your care model to additional populations, if relevant. [5000
character limit]
6. Is your organization currently or formerly part of, operated, managed, or led by an entity
that is participating in or plans to participate in a CMS initiative listed below? Check all that
apply and enter dates:
Example:
• Kidney Care Choices Model: 1/2022 to 1/2023
• ACO REACH: 1/2022 to present
• Enhancing Oncology Model: 1/2024 to 1/2026
. Enhancing Oncology Model: ______ to _______
. ACO Realizing Equity, Access, and Community Health (ACO REACH) Model: ______ to
_______
. Bundled Payments for Care Improvement (BPCI) Advanced Model: ______ to _______
. Comprehensive Care for Joint Replacement Model: ______ to _______
. ESRD Treatment Choices (ETC) Model: ______ to _______
. Making Care Primary (MCP): ______ to _______
. Comprehensive Kidney Care Choices Model: ______ to _______
. Maryland Total Cost of Care Model: ______ to _______
. Medicare Shared Savings Program (MSSP): ______ to _______
. Primary Care First (PCF): ______ to _______
. Vermont All Payer Model:______ to _______
. Other (Please specify) [[Text box]]: ______ to _______
. None

61
7. I certify that I am applying with a TIN that is enrolled in Medicare Part B and eligible to bill
under the Medicare Physician Fee Schedule (PFS), or that prior to the execution of the
Participation Agreement I will establish a TIN that is enrolled in Medicare Part B and eligible
to bill under the PFS.
Please select one:
. Yes, I certify that I am applying with a TIN that is enrolled in Medicare Part B and eligible
to bill under the PFS.
. Yes, I certify that prior to execution of the Participation Agreement, I will establish a TIN
that is enrolled in Medicare Part B and eligible to bill under the PFS. Help Text to option:
I understand that if I do not establish a Medicare Part B TIN that is eligible to bill under
the PFS prior to execution of the Participation Agreement, my organization will not be
able to participate in the Model.
. I cannot certify that I am applying with a TIN, or that I will establish a TIN prior to
execution of the Participation Agreement, that is enrolled in Medicare Part B and eligible
to bill under the PFS.
8. I certify that my organization is a recognized legal entity formed under applicable state,
federal, or tribal law and authorized to conduct business in each state in which it operates.
. Yes.
8a. Attach a copy of a certificate of incorporation or other documentation that demonstrates
that the applicant is recognized as a legal entity by the state in which it is located. [Allow
attachments]
9. To the best of your knowledge, has your organization, your organization’s parent company,
or anyone employed by your organization or parent company had a final adverse legal
action (as defined on page 11 of the
Medicare Enrollment Application for Physicians and
Non-Physician Practitioners, CMS-855i) or been the subject of an investigation by,
prosecution by, or settlement with the Health and Human Services Office of the Inspector
General, U.S. Department of Justice, or any other Federal or State enforcement agency in
the last five years relating to allegations of failure to comply with applicable Medicare or
Medicaid billing rules, the Anti-Kickback Statute, the physician self-referral prohibition, or
any other applicable fraud and abuse laws? Failure to disclose could be grounds for
application denial or immediate termination from the initiative.
. Yes
. No
9a. If yes, please explain the legal actions, investigations, prosecutions, and/or settlements; the
agency involved; and the resolution, if any. [3000 character limit]
10. Please check here to opt out of consideration for the GUIDE safety net provider designation
for infrastructure payment consideration per the definition provided in the RFA. (Optional)
. Yes, I wish to opt out of consideration for the GUIDE safety net provider designation.
62
Ownership Interest
11. Please complete the “Ownership” attachment to provide CMS with a full and complete
understanding of the ownership interests in the applicant, as well as the ownership interests
in the entities with an ownership interest in the applicant. Each party with at least 5%
ownership interest in the applicant should be listed.
*If the privately held company with an ownership or control interest in the applicant is a
subsidiary of another privately held company, please list the parent company(ies) and
ownership interests in that privately held company.
Organization Contacts (Tab 2)
This section asks for organization contact information. Please use the explanations provided to identify
the most appropriate person for each contact field and enter their most current contact information.
If the applicant has a program director who will have primary accountability for implementing the
dementia care program, please include it here.
1. For Primary Application Contact/Secondary Application Contact (Optional)/Program Director
(Optional)
First Name:
Last Name:
Title/Position:
Contact Type: (Primary/Secondary/Program Director)
Phone Number:
Email Address:
Street Address:
City:
State:
ZIP Code:
Complete Application (Section 2)
Staffing and Interdisciplinary Care Team (Tab 1)
1. Describe the interdisciplinary team(s) that the applicant organization will use to deliver
services under the GUIDE Model, including the number and types of staff members and
whether members of the team will be co-located or spread across multiple locations. Please
specify whether the interdisciplinary team currently includes a care navigator and where
staff will need to be hired, and include a hiring plan for these identified staff. Responses
should enable application reviewers to determine whether and how the applicant will meet
the interdisciplinary care team requirements described in the Care Delivery section of the
RFA. [5000 character limit]
63
2. Describe the training that your organization currently provides for staff that deliver care to
people with dementia and their caregivers. If the organization does not currently provide
training, please describe how the organization will meet the care navigator training
requirements. Describe whether and how the applicant will modify this training to meet the
care navigator training requirements of the GUIDE Model, as described in the Care
Navigator Requirements listed in the RFA. [5000 character limit]
3. Does your organization plan to partner with a Medicare Part A or Part B enrolled health care
organization, identified by a different Taxpayer Identification Number or CMS Certification
Number (CCN), such as a physician practice, federally qualified health center, home health
provider, or occupational or physical therapy practice, to meet the Model’s care delivery
requirements?
. Yes
. No
4. Complete the attachment to submit the applicant organization’s Proposed GUIDE
Practitioner Roster, including all historic TINs that any practitioner has used to bill for
Medicare services in the two years prior to November 17, 2023. [Allow attachments]
Note: This is optional, but to be eligible for the Established Program track or designated a
safety net provider under the New Program Track, at time of application the applicant must
provide a Proposed GUIDE Practitioner Roster with the historical TIN(s) under which the
practitioner(s) on their Proposed GUIDE Practitioner Roster have previously billed for Part B
services (see section the Infrastructure Payment section of the RFA).
5. Complete the attachment to submit the applicant organization’s Proposed GUIDE Partner
Organization Roster, including the organization’s TIN. [Allow attachments]
Care Delivery (Tab 2)
The following questions are about your organization’s care delivery methods. Answer each question as
carefully and accurately as possible, based on the current and planned activities if you are accepted to
participate in the GUIDE Model. Your responses will help to determine whether your organization is
assigned to the established program track or the new program track.
1. Has your organization, through an interdisciplinary team that includes at a minimum a care
navigator and a clinician with dementia proficiency, provided any of the following services
to people with dementia for the past 12 months or longer? (check all that apply):
. Comprehensive assessment
. Care planning
. 24/7 access
. Ongoing monitoring and support
. Care coordination and transitional care management
64
. Referral and coordination of services and supports
. Medication management and reconciliation
. Caregiver education and support
. Respite services (including in-home respite, adult day centers, and respite in a 24-hour
facility)
. None of the above
2. For each of the nine GUIDE Care Delivery Service domains, describe in detail:
• Whether and how the applicant organization currently provides these services,
• If the applicant organization currently provides some form of these services,
whether and how their service provision will need to evolve to meet Model
requirements,
• If the applicant organization does not currently provide these services, how it plans
to meet these requirements by the start of the Model performance period.
Responses should enable application reviewers to understand which services will be
provided by the GUIDE Participant versus a Partner Organization. Responses should also
describe the care setting and modality (e.g., in-office, in-home, virtual) that will be used to
deliver the activities under each care delivery domain. Review and address the detailed care
delivery requirements in Appendix B of the Request for Applications in your responses.
• Comprehensive assessment [Text Box, 3000 character limit]
• Care planning [Text Box, 3000 character limit]
• 24/7 access [Text Box, 3000 character limit]
• Ongoing monitoring and support [Text Box, 3000 character limit]
• Care coordination and transitional care management [Text Box, 3000 character
limit]
• Referral and coordination of services and supports [Text Box, 3000 character limit]
• Medication management and reconciliation [Text Box, 3000 character limit]
• Caregiver education and support [Text Box, 3000 character limit]Respite services
(including in-home respite, adult day centers, and respite in a 24-hour facility) [Text
Box, 3000 character limit]
3. Describe how you will affect outcomes for your target beneficiary population through
participation in the GUIDE Model. How will you ensure ongoing quality improvement
throughout the GUIDE Model’s performance period and address the Model’s goals? [Text
Box, 3000 character limit]
Alignment (Tab 3)
1. Describe the population of people with dementia that the applicant organization
currently serves. This should include geographic service area, sociodemographic
characteristics, type and/or stage of dementia, number of people currently served, and
65
referral source, i.e., how the applicant organization identifies people to receive
services. [Text box, 3000 character limit]
2. Estimate the number of Medicare Fee-for-Service beneficiaries with dementia that the
applicant organization intends to serve per year under the GUIDE Model. [Text Box,
numeric values only]
3. Describe how the applicant plans to identify and recruit beneficiaries and caregivers
through voluntary alignment over the course of the Model. [[Note: Please include
experience of the applicant in engaging caregivers and people living with dementia in
their care as well as an overview of marketing and communication plans that the
applicant has for recruitment. Also, include the safeguards the applicant has
implemented or will implement to ensure that, in conducting voluntary alignment
activities, the applicant does not coerce a beneficiary into voluntary alignment or
involuntary exclusion, and to otherwise ensure that beneficiary freedom of choice is
honored.]] [Text Box, 5000 character limit]
Health Equity (Tab 4)
1. Describe your organization’s role in improving health equity among your beneficiary
population. [Text Box, 3000 character limit]
2. Describe your organization's historical or planned processes in engaging underserved
populations. Note: Applicant should include engagement processes through
community outreach, program materials such as translated materials, partnerships
with community-based organizations, or other materials, and results on engagement
where relevant. [Text Box 3000 character limit]
Health Information Technology (Tab 5)
Please select one of the following:
. I certify that my organization will be able to adopt and maintain the health IT needed to
meet the CEHRT definition at 42 CFR 414.1305 by the first performance year as referenced
under the Participation Requirements section of the RFA.
. I am unsure if my organization will be able to adopt and maintain the health IT needed to
meet the CEHRT definition at 42 CFR 414.1305 by the first performance year as referenced
under the Participation Requirements section of the RFA.
. My organization will not be able to adopt and maintain the health IT needed to meet the
CEHRT definition at 42 CFR 414.1305 by the first performance year as referenced under the
Participation Requirements section of the RFA.
66
Applicant Service Area (Tab 6)
Please complete and submit the Excel template to identify, by 5-digit zip-code, the service area from
which your organization will accept patients. If you are selected to participate in the GUIDE Model, CMS
will use this service area data to identify beneficiaries who will receive outreach letters that list your
organization as an available dementia care provider in their area (see the Beneficiary Outreach and
Engagement section of the RFA for more information). [Require attachment]

67
Appendix B: Care Delivery Requirements
1
Comprehensive
Assessment
1.1 Comprehensive Assessment:
1.1.1 GUIDE Participant shall deliver a comprehensive assessment of, and care
planning for, the beneficiary with dementia in accordance with the requirements
below.
1.1.2 Frequency:
1.1.2.1 GUIDE Participant shall perform a comprehensive assessment of the
beneficiary. The comprehensive assessment will initiate the model intervention
and serve as the initial model visit.
1.1.2.2 GUIDE Participant shall complete a new comprehensive assessment
under the terms of Section 1.1 for any beneficiaries that the GUIDE Participant
may have previously assessed as a patient prior to the beneficiary voluntarily
aligning with the GUIDE Participant for purposes of this Model.
1.1.2.3 After the initial comprehensive assessment, GUIDE Participant shall
perform a comprehensive assessment of the beneficiary at least once every
twelve months.
1.1.2.4 The GUIDE Participant has the discretion to re-assess the beneficiary
more frequently; however, the GUIDE Model will only accept data from
reassessments once every one hundred and eighty days.
1.1.3 Modality:
1.1.3.1 An assessment may be performed via telehealth or in-person in the care
team’s office or other outpatient home or domiciliary based on the preference of
the beneficiary and/or caregiver.
1.1.3.2 The assessment shall be administered by appropriate members of the
interdisciplinary care team according to their license and scope of practice.
1.1.4 Required Domains:
1.1.4.1 Clinical:
1.1.4.1.1 Cognition-focused evaluation including a pertinent history and
examination;
1.1.4.1.2 Evaluation of medical decision-making of moderate or high
complexity;
1.1.4.1.3 Functional assessment (e.g., Basic and Instrumental Activities of
Daily Living);
1.1.4.1.4 Screening, or referral to screening, for hearing loss;

68
1.1.4.1.5 Use of standardized instruments for staging of dementia;
1.1.4.1.6 Medication reconciliation and review.
1.1.4.2 Behavioral Health and Psychosocial Needs:
1.1.4.2.1 Evaluation of beneficiary with dementia for behavioral health
needs, including screening for depression, anxiety, substance use, and suicidal
ideation;
1.1.4.2.2 Evaluation of safety, including, but not limited to, environmental,
driving, wandering, fall risk, and abuse, neglect and exploitation.
1.1.4.3 Health-Related Social Needs:
1.1.4.3.1 Screening of beneficiary’s health-related social needs in
accordance with the requirements detailed in the “Health Equity Strategy”
section of this RFA.
1.1.4.4 Advance Care Planning:
1.1.4.4.1 Development, revision, and/or review of an Advance Care Plan
and a Physician Order for Life-Sustaining Treatment (POLST) if available and
beneficiary wishes to complete.
1.1.4.5 Coordination:
1.1.4.5.1 Identification of beneficiary’s primary care provider, behavioral
health provider, and specialty provider(s), if any, and coordination services to
manage the beneficiary’s dementia and any co-occurring conditions.
1.1.4.5.2 Identification of any community-based services and supports, and
home and community-based services that the beneficiary is receiving.
1.2 Caregiver Assessment: GUIDE Participant shall deliver an assessment of the
beneficiary’s caregiver in accordance with the requirements hereinbelow.
1.2.1 GUIDE Participant shall identify the beneficiary’s caregiver(s) and their ability
and willingness to assume, or to continue to furnish, assistance.
1.2.2 GUIDE Participant shall assess the caregiver’s knowledge, needs, and social
supports, and assess the caregiver’s well-being, stress level, and other challenges.
1.2.3 If the beneficiary does not have a caregiver, the GUIDE Participant shall make a
reasonable effort to help identify a caregiver for the beneficiary.
1.2.3.1 If the GUIDE Participant and the beneficiary are not able to locate a
caregiver for the beneficiary, then Section 1.2: Caregiver Assessment and Section
8: Caregiver Education and Support do not apply to that beneficiary, and instead
the GUIDE Participant shall make additional efforts and put safeguards into its
care delivery to support the beneficiary continuing to reside in the community.

69
1.3 Home Visit Assessment:
1.3.1 For beneficiaries in the low complexity dyad tier or low complexity individual
tier: GUIDE Participant may, but is not required to, visit the beneficiary and, if
applicable, his or her caregiver in person at the current residence of the beneficiary.
If the GUIDE Participant does not visit the beneficiary in person, the visit may be
performed remotely through electronic means. For beneficiaries in moderate or high
complexity dyad tiers, or moderate to high complexity individual tier: GUIDE
Participant shall visit the beneficiary and, if available, his or her caregiver at the
current residence of the beneficiary. If the caregiver or other members of the care
team are not present, the GUIDE Participant may facilitate participation of the
caregiver and other members of the care team by enabling such individuals to
participate in the visit remotely through electronic means.
1.3.2 The home visit with the beneficiary should occur within two months after the
initial assessment and can be performed by any member of the interdisciplinary care
team.
1.3.3 During the home visit, the GUIDE Participant shall assess the following: i) safety
of the home environment and the beneficiary’s ability to navigate and manage the
home environment, ii) beneficiary’s function in activities of daily living, and iii) other
environmental, social, and behavioral factors that might impact the function and
needs of the beneficiary and their caregiver.
2
Care Plan
2.1 Based on findings from the comprehensive initial assessment, including the HRSN
screening, home visit, and guidance from the beneficiary and the caregiver, the
GUIDE Participant shall develop elements of the person-centered care plan with
recommendations for i) addressing the beneficiary’s goals, strengths, preferences and
needs, ii) the required domains of the comprehensive assessment, iii) the
coordination of community-based services and supports, including respite services if
applicable, and a listing of recommended service providers and which individual or
program is responsible for payment of each service provider, and iv) the caregiver’s
education and support services.
2.2 The initial care plan and future revisions shall be led by the beneficiary. At the
discretion of the beneficiary and as appropriate to the individual, the GUIDE
Participant may also incorporate input from the beneficiary’s caregiver. The GUIDE
Participant shall share the initial care plan and future revisions with the beneficiary
and their caregiver along with any relevant education, supports, and other resources,
to carry out the goals of the plan.
2.3 The GUIDE Participant shall modify the written care plan as needed, or requested, to
reflect the beneficiary’s changing circumstances, goals, preferences, and needs.
2.4 The person-centered care plan shall be incorporated into the beneficiary’s electronic
health record and shared with the beneficiary’s primary care provider (if the
beneficiary’s primary care provider is not a member of the GUIDE Participant’s care

70
team) and any specialist or other provider in accordance with Section 5, Care
Coordination and Transitional Care Management.
3
24/7 Access
3.1 GUIDE Participant shall provide either (i) 24/7 access to an interdisciplinary care team
member or (ii) maintain a 24/7 helpline that the beneficiary and/or their caregiver
may call to speak with either a member of the care team or a third party engaged by
the GUIDE Participant to provide communication with human support (e.g., not
artificial intelligence) during off-duty hours. A third party engaged by the GUIDE
Participant to provide communication during off-duty hours shall share with the
interdisciplinary care team information of any communication with a beneficiary
and/or their caregiver.
3.2 If the GUIDE Participant uses a 24/7 helpline, the 24/7 helpline shall be available to
receive ad hoc one-on-one support calls from the caregiver (see Section 8.2.4).
4
Ongoing
Monitoring and
Support
4.1 The care navigator shall be the primary point of contact for the beneficiary and their
caregiver.
4.2 The care navigator shall provide ongoing contact with the beneficiary and/or
caregiver in order to revise and maintain the person-centered care plan as needed
(see Section 2), identify unmet needs and coordinate clinical and community-based
services and supports (see Section 6), monitor medication management and
adherence (see Section 7), and provide caregiver education and support (see Section
8) as may be needed to support the beneficiary and their caregiver.
4.2.1 If the care navigator is a non-clinical professional, the care navigator should
consult with the care team’s clinical team members for any medical or other issues
that present with complexity.
4.3 Frequency: GUIDE Participant shall maintain a minimum contact frequency with the
beneficiary and/or their caregiver. Minimum contact requirements vary by model tier,
as follows:
4.3.1 Beneficiaries with a caregiver
o
o
o
Low complexity dyad tier: at least quarterly
Moderate complexity dyad tier: at least once a month
High complexity dyad tier: at least once a month
4.3.2 Beneficiaries without a caregiver
o
o
Low complexity individual tier: at least once a month
Moderate to high complexity individual tier: at least twice a month
4.4 Modality: GUIDE Participant may provide ongoing contact in-person (in-clinic or in-
home), by phone, and/or by audio-visual modalities in accordance with the
beneficiary’s and/or caregiver’s preferences, as applicable. Short Messaging Service
(SMS) may not be used to contact the beneficiary or caregiver to meet the minimum
contact frequency, but can be used, with the beneficiary’s and caregiver’s consent, in
other communications.

71
5
Care
Coordination
and Transitional
Care
Management
5.1 If the beneficiary’s primary care provider is not a member of the GUIDE Participant’s
care team, GUIDE Participant shall coordinate with the beneficiary’s primary care
provider and notify the beneficiary’s primary care provider that the beneficiary is
participating in a dementia care management program and ensure that the primary
care provider has access to the beneficiary’s care plan and any updated/revised care
plans.
5.2 GUIDE Participant may refer the beneficiary to a specialist or other provider to
address any physical or behavioral health (such as, mental health or substance use)
co-occurring conditions of the beneficiary. GUIDE Participant may notify the specialist
or other provider that the beneficiary is participating in a dementia care management
program and send the specialist or other provider the beneficiary’s person-centered
care plan, and any updated/revised care plans, by electronic health record, fax, or
mail. The GUIDE Participant shall also notify the beneficiary’s primary care provider of
the referral to a specialist and/or other provider. If the primary care provider is
actively co-managing the beneficiary, the GUIDE Participant should make this referral
in consultation with the primary care provider. The dementia care team must close
the referral loop with the specialist by ensuring they receive documentation from the
beneficiary’s visit and any changes to their care plan.
5.3 If the GUIDE Participant refers the beneficiary to a specialist or other provider, a
member of the care team shall introduce the beneficiary to the new provider if
requested by the beneficiary and/or their caregiver so that the new provider is aware
of the patient history and can share recommendations with the care team for
incorporation into the care plan.
5.4 GUIDE Participant shall provide care coordination services, medication
management/reconciliation, and support to the beneficiary in transitions between
their personal residence and care settings, such as a hospital, emergency department,
nursing facility, and/or hospice.
5.5 GUIDE Participant shall provide additional care coordination services needed to help
manage the beneficiary’s dementia and co-occurring conditions, if any, across the
care-continuum.
6
Referral and
Coordination of
Services and
Supports
6.1 GUIDE Participant shall i) refer and connect beneficiaries and their caregivers to
community-based services and supports that address the common needs of persons
with dementia and their caregivers (e.g., home-delivered meals, adult day centers,
personal care, environmental modifications, contractors, food banks), and/or ii) enter
into a written agreement with a local Area Agency on Aging or a Tribal Aging Program
(funded through Title VI of the Older Americans Act) requiring that the local Area
Agency on Aging or Tribal Aging Program assists beneficiaries and their caregivers
with coordinating community-based services and supports.
6.2 If the beneficiary is eligible for and receiving home- and community-based services
(HCBS) through a state Medicaid program, the GUIDE Participant shall contact and
attempt to coordinate the delivery of community-based services and supports and
HCBS with the beneficiary’s waiver/HCBS program case manager. Coordination

72
between the GUIDE Participant and the beneficiary’s waiver/HCBS program case
manager shall include sharing information about the GUIDE Model and reviewing the
services that the beneficiary receives through both the GUIDE Model and Medicaid
for the purpose of understanding gaps or duplication in the beneficiary’s care.
6.3 GUIDE Participant shall join or maintain a community referral inventory system that
includes resources for the health-related social needs screened as part of the
comprehensive assessment (see Section 1.1.4.3), and the care navigator shall refer
and connect the beneficiary and their caregiver to resources relevant to their needs.
6.4 GUIDE Participant shall maintain, or have access to, an inventory of community-based
resources for services and supports that address the common needs of persons with
dementia and their caregivers (e.g., home-delivered meals, adult day centers,
personal care, environmental modification, contractors, food banks) and as
appropriate, share these resources with the beneficiary and their caregiver.
7
Medication
Management
and
Reconciliation
7.1 A clinician with prescribing authority shall review and reconcile the medications that
beneficiary is taking at the time of the comprehensive initial assessment, at any
additional future assessments, and then periodically as requested by other members
of the care team, the beneficiary or the caregiver, as appropriate. Medication review
would customarily include, as part of this element, a review of prescription drugs,
over-the-counter medications, supplements, natural treatments, and/or any other
substances the beneficiary might be using for any purpose.
7.2 If clinically advisable for the beneficiary, GUIDE Participant’s advanced practice nurse,
physician assistant, or physician shall consider prescribing medications that are
beneficial for the beneficiary.
7.3 If clinically advisable for the beneficiary, GUIDE Participant’s advanced practice nurse,
physician assistant, or physician shall de-prescribe any medications that are
inappropriate for the beneficiary to continue taking.
7.4 GUIDE Participant shall share recommended changes to the beneficiary’s medications
with the beneficiary’s primary care provider and other medical specialists, as
applicable, and confirm that the relevant medical provider, either the primary care
provider or the medical specialist, agrees to the proposed change to the beneficiary’s
medications prior to the beneficiary changing their medications.
7.5 GUIDE Participant’s care navigator shall provide information on supports to help the
beneficiary maintain the correct medication schedule, such as pill reminders, pill
boxes, and/or software applications.
8.1 In order to provide education and support to the caregiver of a beneficiary, GUIDE
Participant shall administer a caregiver support program, which is based on the
caregiver assessment referred to in Section 1.2 and is responsive to ongoing
caregiver needs.
8.2 The caregiver support program shall offer the following services:

73
8
Caregiver
Education and
Support
8.2.1 Caregiver skills training: GUIDE Participant shall provide the caregiver with the
option to receive training to help the beneficiary continue to live as safely and
comfortably as possible in the community. The training shall include the following
topics: emergency services, safety in the home, assistance with activities of daily
living (ADL) and instrumental ADLs, responding to and managing the beneficiary’s
behavioral and psychosocial symptoms, identifying and obtaining help across the
care continuum, working with health care and other community-based providers,
recreation, social and leisure activities, making plans for the future, and caregiver
self-care and stress management.
8.2.2 Dementia diagnosis information: If beneficiary and/or caregiver wish to
receive further information regarding the beneficiary’s dementia diagnosis, GUIDE
Participant shall speak with and provide written educational materials to the
caregiver regarding the beneficiary’s dementia diagnosis. These materials may
include, but are not limited to, information on dementia, common behavioral
changes, functional status, and resources available publicly and through the GUIDE
Participant. These materials should be comprehensible to a lay person and in the
primary language spoken by the beneficiary and the caregiver.
8.2.3 Support group services: GUIDE Participant shall provide the caregiver with the
option to participate in a group setting where a facilitator trained in dementia and
caregiving shall work with caregivers on self-care, home safety, caregiver skills,
personal care, and managing challenging behaviors.
8.2.4 Ad hoc one-on-one support calls: GUIDE Participant shall be available for one-
on-one support calls with the caregiver to address issues in furnishing care and
support to the beneficiary as the issues arise. For example, these calls may focus on
the caregiver’s needs and goals by coaching caregivers on stress management, self-
care and well-being behaviors, and how to identify and address behavioral
challenges and functional status of the beneficiary with dementia, and support safety
of the caregiver, and the beneficiary. The calls may be initiated by the beneficiary,
the caregiver, or the GUIDE Participant. The GUIDE Participant’s requirement to
maintain minimum contact with the beneficiary in accordance with Section 4.3 may
be used to satisfy this requirement for one-on-one support calls.
8.3 Modality: All services may be provided virtually or in-person. In addition, GUIDE
Participant shall deliver the services listed under Section 8.2 as follows:
8.3.1 Caregiver skills training: Must be provided by either a member of the care
team or through a contracted vendor or community organization that is reimbursed
by the GUIDE Participant; may be provided in a one-on-one setting or group format.
8.3.2 Dementia diagnosis information at program entry: Must be provided directly by
a member of the care team in a one-on-one setting.
8.3.3 Support group services: May be provided directly by a member of the care
team, through a contracted vendor or community organization that is reimbursed by
the GUIDE Participant, or through referral to a community organization that offers
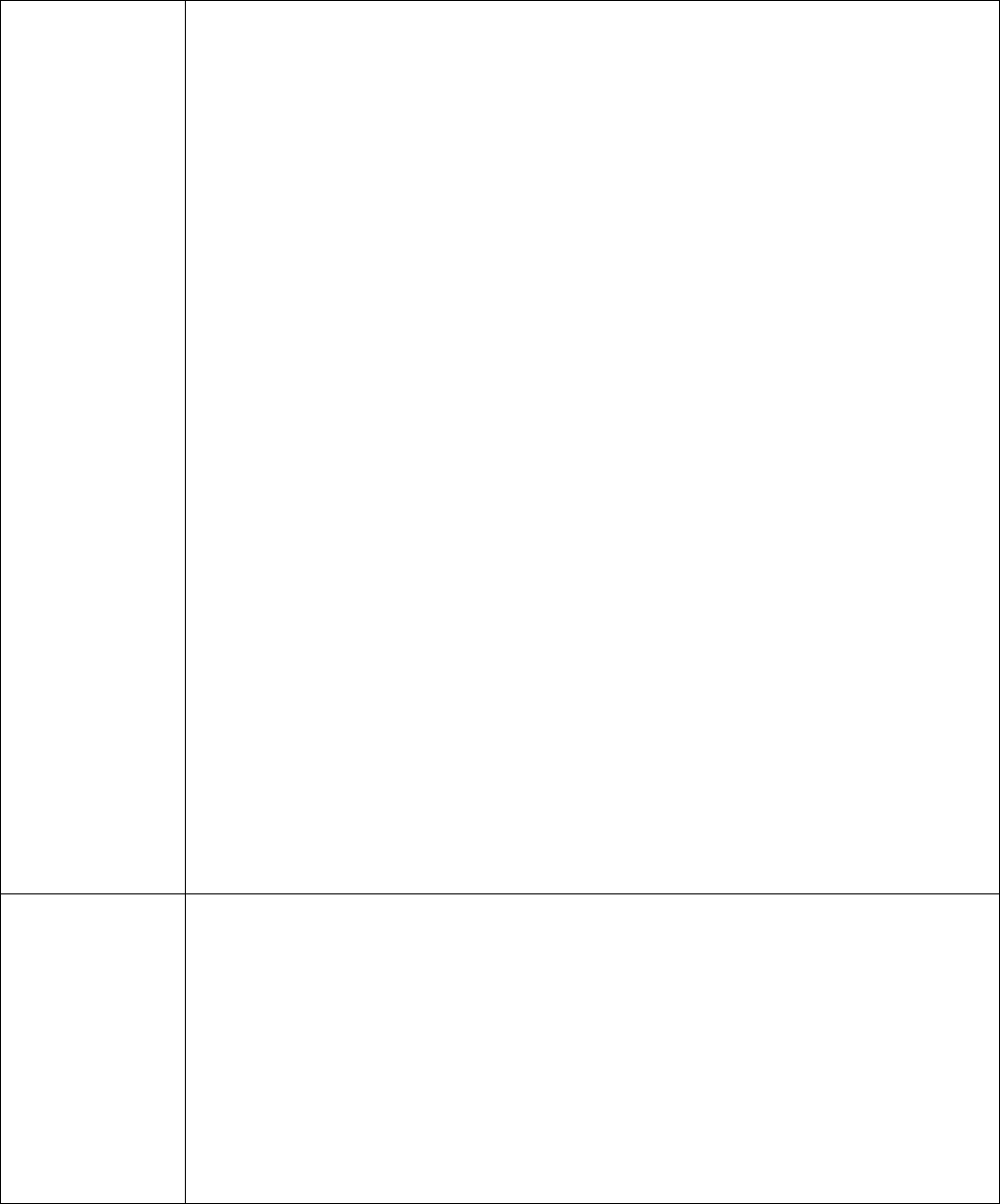
74
support group services to the community free of charge. Beneficiaries with dementia
and caregivers may decline to participate in support groups or change their mind
about participation at any time.
8.3.4 Ad hoc one-on-one support calls: Must be provided directly by a member of
the care team.
8.4 In addition to the required services listed above, the GUIDE Participant should
consider whether to provide the following optional services:
8.4.1 Peer-to-peer support: Experienced caregivers, whose caregiving experience
has come to an end, would provide practical information, and support and mentoring
to the caregiver participating in the Model.
8.4.2 Resources or referrals for self-care and well-being instruction (e.g., group
walks, meditation classes): Specialized services centered around caregiver stress and
health management. Services could include, but are not limited to, mindfulness and
relaxation techniques, cognitive behavioral therapy, musical and arts classes, and
exercise classes.
8.4.3 Assist with education on the role of the caregiver: Information on the
traditional responsibilities of a caregiver for a person living with dementia and the
resources available to them through the GUIDE Participant.
8.4.4 Accessing community-based resources: Coaching the caregiver on how to
access community-based resources relevant to their caregiving role, such as
transportation, nutrition support, homemaker/yard services. This service is in
addition to the referral support provided under Section 6 Referral and Coordination
of Services and Supports.
8.5 Psychological counseling referral: The caregiver may work with a specialist on
developing new behaviors or strategies to help address caregiving demands,
identifying areas for improvement for the beneficiary-caregiver dyad, or assistance in
addressing depression, anxiety, and suicidal ideation in the caregiver and/or the
beneficiary.
9
Respite
9.1 GUIDE Participant shall provide GUIDE Respite Services to beneficiaries who qualify
for respite under the Model and choose to receive respite. GUIDE Respite Services are
furnished based on the beneficiary’s qualifying status. GUIDE Participants and eligible
beneficiaries shall decide how much GUIDE Respite Services the beneficiary will
receive taking into consideration the beneficiary’s need for GUIDE Respite Services
and the capped amount of GUIDE Respite Services covered under the Model.
9.2 GUIDE Participant shall provide in-home GUIDE Respite Services directly or contract
with at least one provider of in-home respite services. The contract must specify how
the GUIDE Participant will reimburse the respite provider for Respite Services
rendered to eligible beneficiaries.

75
9.3 GUIDE Participant may also contract with adult day centers or facilities that can
provide 24-hour care to deliver GUIDE Respite Services in these settings to eligible
beneficiaries.

76
Appendix C: Example Patient Assessment and Alignment Form
Example GUIDE Patient Assessment and Alignment Form
Results from (check one):
. Initial Assessment . Re-assessment . Re-assessment due to new primary caregiver
Date of assessment: ____________
Patient first name: ________ Patient middle name:(if applicable) ______ Patient last name: _________
Patient Address: _______________ Email: _______________ Phone Number: _______________
Patient resides in: . home . assisted living facility . memory care program (excludes nursing home
level of care)
Patient Date of Birth: ___/___/_____
Patient Medicare Beneficiary Identifier: __________
Patient Medicaid ID number: _____________ (as applicable)
Patient dementia stage: (Drop-down menu: CDR, FAST): ___ (enter numerical score)
Does patient have a caregiver, defined as a relative, or an unpaid nonrelative, who assists the
beneficiary with activities of daily living and/or instrumental activities of daily living? (Drop-down menu:
yes-multiple, yes-one, no, undetermined)
If yes:
Caregiver first name: __________ Caregiver last name: ___________
Caregiver Address: _______________ Email: _______________ Phone Number: _______________
What is primary caregiver’s relationship to patient? (Drop-down menu: spouse, child, non-immediate
family member, friend, other)
Does primary caregiver live with patient? (Drop-down menu: yes, no)
Is primary caregiver a Medicare beneficiary? (Drop-down menu: yes, no)
If yes, what is the primary caregiver’s Medicare Beneficiary Identifier: __________
Primary caregiver Zarit Burden Interview score: ___ (enter numerical score as a whole number)
In my clinical judgment, the assessed beneficiary meets the National Institute on Aging-Alzheimer’s
Association diagnostic guidelines for dementia and/or the DSM-5 diagnostic guidelines for major
neurocognitive disorder, or I have received a written report (electronic or hard-copy) of a documented
dementia diagnosis from another Medicare qualified health professional.
.
.
Yes
No
77
Attesting clinician:
First name: ____________ Middle Name:_____________ Last name: ____________
National Provider Identification (NPI): ____________
Patient referral source:
. Referred by a healthcare provider . Referred by a community-based organization . Self-referral
