
Drug Distribution and Control: Preparation and Handling–Guidelines 91
ASHP Guidelines on Quality Assurance
for Pharmacy-Prepared Sterile Products
Patient morbidity and mortality have resulted from incor-
rectly prepared or contaminated pharmacy-prepared
products.
1–7
Pharmacists seldom know that inaccurate
or contaminated products are dispensed when pharmacy
quality monitors are inadequate.
8–10
In contemporary health
care organizations, more patients are receiving compounded
sterile products that are stored for extended periods before
use (allowing the growth of a pathological bioload of micro-
organisms
11
), more patients are seriously ill, and more patients
are immunocompromised than ever before.
These ASHP guidelines are intended to help pharmacists
and pharmacy technicians prepare sterile products of high
quality.
a
The pharmacist is responsible for compounding and
dispensing sterile products of correct ingredient identity, purity
(freedom from physical contaminants, such as precipitates,
12
and
chemical contaminants), strength (including stability
13
and com-
patibility), and sterility and for dispensing them in appropriate
containers, labeled accurately and appropriately for the end user.
Other professional organizations have published useful
guidelines on compounding and dispensing sterile products.
The United States Pharmacopeia (USP) publishes the offi-
cial compendium The United States Pharmacopeia and The
National Formulary (USP) and its supplements, all of which
may have legal implications for pharmacists.
14,15
The reader
would especially benefit from studying the USP general infor-
mation chapter on sterile drug products for home use,
13
which
is referred to often in this ASHP guideline. The National
Association of Boards of Pharmacy (NABP) has published
less detailed model regulations for use by state boards of phar-
macy.
16,17
The American Society for Parenteral and Enteral
Nutrition (A.S.P.E.N.) recently published a special report on
safe practices for parenteral nutrition formulations.
18
Other governmental and accreditation sources are
more general. The Joint Commission on Accreditation of
Healthcare Organizations (JCAHO) publishes at least four
sets of standards that mention pharmacy compounding. The
hospital accreditation standards simply state that the organi-
zation adheres to laws, professional licensure, and practice
standards governing the safe operation of pharmaceutical
services.
19
The JCAHO home care standards require that
medications be safely prepared, including “using appropri-
ate techniques for preparing sterile and nonsterile medications
and products.” For example, the home care standards state
that “appropriate quality-control techniques are used to check
for preparation accuracy and absence of microbial contamina-
tion. Techniques for preparing sterile products follow guide-
lines established by the American Society of Health-System
Pharmacists.”
20
The JCAHO standards for long-term-care
pharmacies list important conditions for product preparation,
such as separate areas for sterile product preparation, use of a
laminar-airflow workbench or class 100 cleanroom, and quality
control systems to ensure the accuracy and sterility of final
products.
21
The JCAHO standard for ambulatory care infusion
centers states, among other things, several facility-related stan-
dards, for example the use of biological safety cabinets to pro-
tect personnel preparing cytotoxic or hazardous medications;
work surfaces free of equipment, supplies, records, and labels
unrelated to the medication being prepared; and a separate area
for preparing sterile products that is constructed to minimize
opportunities for particulate and microbial contamination.
22
The Food and Drug Administration (FDA) publishes
regulations on current good manufacturing practices that
apply to sterile products made by pharmaceutical manufac-
turers for shipment in interstate commerce. Pursuant to the
FDA Modernization Act of 1997 (FDAMA), Section 503A
of the Food, Drug, and Cosmetic Act states that pharmacy
compounding must comply with an applicable USP mono-
graph, if one exists, and the USP chapter on pharmacy com-
pounding
14
or be a component of an FDA-approved drug
product; or, if neither of these apply to the ingredient being
compounded, the substance must appear on a list of bulk
drug substances developed by FDA and must be accompa-
nied by a valid certificate of analysis and be manufactured
in an FDA-registered establishment.
23
Inactive ingredients
compounded by licensed pharmacies must comply with
applicable USP monographs, if they exist, and the USP
chapter on pharmacy compounding.
14
FDAMA prohibits
pharmacists from compounding drug products that appear
on a list of products that have been withdrawn or removed
from the market because they have been found unsafe or
ineffective. FDAMA also says that pharmacists may not
compound, regularly or in inordinate amounts, drug prod-
ucts that are essentially copies of commercially available
drug products; nor may they compound drug products iden-
tified by regulation as presenting demonstrable difficulties
for compounding that reasonably demonstrate an adverse
effect on safety or effectiveness.
The Centers for Disease Control and Prevention (CDC)
has published guidelines for hand washing, prevention of intra-
vascular infections, and hospital environmental control.
24,25
The ASHP Guidelines on Quality Assurance for Pharmacy-
Prepared Sterile Products are applicable to pharmaceutical ser-
vices in various practice settings, including, but not limited to,
hospitals, community pharmacies, nursing homes, ambulatory
care infusion centers, and home care organizations. ASHP has
also published practice standards on handling cytotoxic and
hazardous drugs
26
and on pharmacy-prepared ophthalmic pro-
d ucts.
27
These ASHP guidelines do not apply to the manufac-
ture of sterile pharmaceuticals as defined in state and federal
laws and regulations, nor do they apply to the preparation of
medications by pharmacists, nurses, or physicians in emer-
gency situations for immediate administration to patients (e.g.,
cardiopulmonary resuscitation). All guidelines may not be ap-
plicable to the preparation of radiopharmaceuticals.
These guidelines are referenced with supporting sci-
entific data when such data exist. In the absence of published
supporting data, guidelines are based on expert opinion or
generally accepted pharmacy procedures. Pharmacists are
urged to use professional judgment in interpreting these
guidelines and applying them in practice. It is recognized
that, in certain emergency situations, a pharmacist may be
requested to compound products under conditions that do
not meet these guidelines. In such situations, it is incumbent
upon the pharmacist to employ professional judgment in

92 Drug Distribution and Control: Preparation and Handling–Guidelines
weighing the potential patient risks and benefits associated
with the compounding procedure in question.
Objectives. The objectives of these guidelines are to provide
1. Information on quality assurance and quality control
activities that should be applied to the preparation of
sterile products in pharmacies and
2. A method to match quality assurance and quality con-
trol activities with the potential risks to patients posed
by various types of products.
Multidisciplinary Input. Pharmacists are urged to participate
in the quality or performance improvement, risk management,
and infection control programs of their health care organiza-
tions, including developing optimal sterile product procedures.
Definitions. Definitions of selected terms, as used in this
document, are provided in Appendix A. For brevity in this
document, the term quality assurance will be used to refer
to both quality assurance and quality control (as defined in
Appendix A), as befits the circumstances.
Risk-Level Classification
In this document, sterile products are grouped into three
levels of risk to the patient, increasing from least (level
1) to greatest (level 3) potential risk based on the danger
of exposing multiple patients to inaccurate ingredients or
pathogens and based on microbial growth factors influenced
by product storage time, temperature and product ability
to support microbial growth, surface and time exposure of
critical sites, and microbial bioload in the environment. When
circumstances make risk-level assignment unclear, guidelines
for the higher risk level should prevail. Consideration should
be given to factors that increase potential risk to the patient
such as high-risk administration sites and immunocom-
promised status of the patient. A comparison of risk-level
attributes appears in Appendix B.
Risk Level 1. Risk level 1 applies to compounded sterile
products that exhibit characteristics 1, 2, and 3, stated below.
All risk level 1 products should be prepared with sterile
equipment (e.g., syringes and vials), sterile ingredients and
solutions, and sterile contact surfaces for the final product.
Risk level 1 includes the following:
1. Products
a. Stored at room temperature (see Appendix A for
temperature definitions) and completely admin-
istered within 28 hours after preparation or
b. Stored under refrigeration for 7 days or less be-
fore complete administration to a patient over a
period not to exceed 24 hours (Table 1) or
c. Frozen for 30 days or less before complete
administration to a patient over a period not to
exceed 24 hours.
2. Unpreserved sterile products prepared for administra-
tion to one patient or batch-prepared products contain-
ing suitable preservatives prepared for administration
to more than one patient.
3. Products prepared by closed-system aseptic transfer
of sterile, nonpyrogenic, finished pharmaceuticals
(e.g., from vials or ampuls)
b
obtained from licensed
manufacturers into sterile final containers (e.g.,
syringes, minibags, elastomeric containers, portable
infusion-device cassettes) obtained from licensed
manufacturers.
Examples of risk level 1 processes include transferring
a sterile drug product from a vial into a commercially pro-
duced i.v. bag; compounding total parenteral nutrient (TPN)
solutions by combining dextrose injection and amino acids
injection via gravity transfer into a sterile empty container,
with or without the subsequent addition of sterile drug prod-
ucts to the final container with a sterile needle and syringe;
and transferring a sterile, preserved drug product into sterile
syringes with the aid of a mechanical pump and appropriate
sterile transfer tubing device.
Risk Level 2. Risk level 2 sterile products exhibit character-
istic 1, 2, or 3, stated below. All risk level 2 products should
be prepared with sterile equipment, sterile ingredients and
solutions, and sterile contact surfaces for the final product
and with closed-system transfer methods. Risk level 2
includes the following:
1. Products stored beyond 7 days under refrigeration,
stored beyond 30 days frozen, or administered beyond
28 hours after preparation and storage at room tem-
perature (Table 1).
2. Batch-prepared products without preservatives (e.g.,
epidural products) that are intended for use by more
than one patient. (Note: Batch-prepared products with-
out preservatives that will be administered to multiple
patients carry a greater risk to the patients than products
prepared for a single patient because of the potential ef-
fect of inaccurate ingredients or product contamination
on the health and well-being of a larger patient group.)
3. Products compounded by complex or numerous
manipulations of sterile ingredients obtained from
licensed manufacturers in a sterile container or
reservoir obtained from a licensed manufacturer by
using closed-system aseptic transfer; for example, TPN
solutions prepared with an automated compounder.
(Note: So many risks have been associated with
automated compounding of TPN solutions that its
complexity requires risk level 2 procedures.
18
)
Examples of risk level 2 processes include prepar-
ing portable-pump reservoirs for multiday (i.e., ambient
temperature) administration; subdividing the contents of a
bulk, sterile injectable (without preservatives) into sin-
gle-dose syringes; and compounding TPN solutions with
an automated compounding device involving repeated
attachment of fluid containers to proximal openings of the
compounder tubing set and of empty final containers to the
distal opening, the process concluding with the transfer of
additives into the filled final container from individual drug
product containers or from a pooled additive solution.
Risk Level 3. Risk level 3 products exhibit either character-
istic 1 or 2:
1. Products compounded from nonsterile ingredients or
compounded with nonsterile components, containers,
or equipment before terminal sterilization.

Drug Distribution and Control: Preparation and Handling–Guidelines 93
2. Products prepared by combining multiple ingredients—
sterile or nonsterile—by using an open-system transfer
or open reservoir before terminal sterilization.
Examples of risk level 3 products are calcium levu-
linate injection, estradiol in oil injection, and morphine sul-
fate 50-mg/mL injection.
32
Quality Assurance for Risk Level 1
RL 1. 1: Policies and Procedures.
33
Up-to-date policies and
procedures for compounding sterile products should be written
and available to all personnel involved in these activities. When
policies and procedures are changed they should be updated, as
necessary, to reflect current standards of practice and quality.
Additions, revisions, and deletions should be communicated to
all personnel involved in sterile compounding and related ac-
tivities. These policies and procedures should address person-
nel education and training requirements, competency evalu-
ation, product acquisition, storage and handling of products
and supplies, storage and delivery of final products, use and
maintenance of facilities and equipment,
34
appropriate garb and
conduct for personnel working in the controlled area, process
validation, preparation technique,
35
labeling, documentation,
and quality control.
36
Further, written policies and procedures
should address personnel access and movement of materials into
and near the controlled area. Policies and procedures for moni-
toring environmental conditions in the controlled area should
take into consideration the amount of exposure of the product
to the environment during compounding and the environmental
control devices used to create the critical area. Sources of infor-
mation include vendor-supplied inservice programs and multi-
media training programs, such as videotapes and Internet-site
information. Before compounding sterile products, all personnel
involved should read the policies and procedures. Written poli-
cies and procedures are required for all environmental control
devices used to create the critical area for manipulation of sterile
products. Examples of such devices are laminar-airflow work-
stations, biological safety cabinets, class 100 cleanrooms, and
barrier isolator workstations (see Appendix A).
c
RL 1.2: Personnel Education, Training, and Evaluation.
Training is the most important factor in ensuring the qual-
ity of sterile products. Pharmacy personnel preparing or dis-
pensing sterile products must receive suitable didactic and
experiential training and competency evaluation through
demonstration, testing (written or practical), or both. Some
aspects that should be included in training programs include
aseptic technique; critical-area contamination factors; envi-
ronmental monitoring; facilities, equipment, and supplies;
sterile product calculations and terminology; sterile product
compounding documentation; quality assurance procedures;
aseptic preparation procedures; proper gowning and gloving
technique; and general conduct in the controlled area. In
addition to knowledge of chemical, pharmaceutical, and
clinical properties of drugs, pharmacists should be knowl-
edgeable about the principles of pharmacy compounding.
14
Videotapes
37,38
and additional information on the essential
components of a training, orientation, and evaluation pro-
gram are described elsewhere.
39,40
All pharmacy and non-
pharmacy personnel (e.g., environmental services staff)
who work in the controlled area should receive documented
training on cleaning, sanitizing, and maintaining equipment
used in the controlled area. Training should be specific to the
environmental control device and equipment present in the
controlled area and should be based on current procedures.
The aseptic technique of each person preparing sterile
products should be observed and evaluated as satisfactory
during orientation and training and at least annually there-
after.
41
In addition to observation, methods of evaluating the
knowledge of personnel include written or practical tests and
process validation.
42,43
RL 1.3: Storage and Handling within the Pharmacy.
44
Solutions, drugs, supplies, and equipment used to prepare
or administer sterile products should be stored in accordance
with manufacturer or USP requirements. Temperatures in
refrigerators and freezers used to store ingredients and fin-
ished sterile preparations should be monitored and docu-
mented daily to ensure that compendial storage requirements
are met. Warehouse and other pharmacy storage areas where
ingredients are stored should be monitored to ensure that
temperature, light, moisture, and ventilation remain within
manufacturer and compendial requirements. To permit ad-
equate floor cleaning, drugs, supplies, and compounding
equipment should be stored on shelving, cabinets, and carts
above the floor. Products that have exceeded their expiration
dates should be removed from active storage areas. Before
use, each drug, ingredient, and container should be visually
inspected for damage, defects, and expiration date.
45
Unnecessary personnel traffic in the controlled area
should be minimized. Particle-generating activities, such as
removal of intravenous solutions, drugs, and supplies from
cardboard boxes, should not be performed in the controlled
area. Products and supplies used in preparing sterile prod-
ucts should be removed from shipping containers outside the
controlled area before aseptic processing is begun. Packaging
materials and items generating unacceptable amounts of par-
ticles (e.g., cardboard boxes, paper towels [unless lint-free],
reference books) should not be permitted in the controlled
area or critical area. The removal of immediate packaging
designed to retain the sterility or stability of a product (e.g.,
syringe packaging, light-resistant pouches) is an exception;
obviously, this type of packaging should not be removed
outside the controlled area. Disposal of packaging materials,
used syringes, containers, and needles should be performed
Table 1.
Assignment of Products to Risk Level 1 or 2 according to Time and Temperature before Completion
of Administration
No. Days Storage
Risk Level Room Temperature (15–30 °C) Refrigerator (2–8 °C)
Freezer (−20 to −10°C)
1
Completely administered within 28 hr
≤7
≤30
2
Storage and administration exceed 28 hr
>7
>30

94 Drug Distribution and Control: Preparation and Handling–Guidelines
at least daily, and more often if needed, to enhance sanitation
and avoid accumulation in the controlled area. Trash cans
should be below the level of the laminar-airflow workbench
and should be removed from the controlled area before be-
ing emptied. Sharps containers should be safely placed into
the waste stream, according to policies developed by the
institution to comply with regulations of the Occupational
Safety and Health Administration (OSHA).
In the event of a product recall, there should be a
mechanism for tracking and retrieving affected products
from specific patients to whom the products were dispensed.
RL 1.4: Facilities
46
and Equipment.
47
The controlled area
should be a limited-access area sufficiently separated from
other pharmacy operations to minimize the potential for
contamination that could result from the unnecessary flow of
materials and personnel into and out of the area. The controlled
area is a buffer from outside air that is needed because strong
air currents from briefly opened doors, personnel walking
past the laminar-airflow workbench, or the air stream from
the heating, ventilating, and air conditioning system can
easily exceed the velocity of air from the laminar-airflow
workbench. Also, operators introducing supplies into the
laminar-airflow workbench or reaching in with their arms
can drag contaminants from the environment surrounding
the workbench.
15
Cleanliness of the controlled area can be
enhanced by (1) limiting access to those personnel assigned
to work in the controlled area, (2) having those personnel wear
the appropriate garb, (3) donning and removing garb outside
the controlled area, (4) keeping doors to the controlled area
closed, (5) limiting storage in the controlled area to items in
constant use, (6) using low-particulate shelving, counters,
and carts (e.g., stainless steel) in the controlled area, (7) not
allowing cardboard and other particle-generating materials in
the controlled area, (8) controlling the temperature and humid-
ity inside the room, and (9) implementing a regular cleaning
(e.g., nightly floor disinfection) and maintenance schedule.
48
Barrier isolator workstations are closed systems and
are not as sensitive to their external environment as laminar-
airflow equipment. It is good practice to (1) place barrier
isolator workstations in limited-access areas, (2) control the
temperature and humidity of the surrounding area, and (3)
clean and sanitize the surrounding area on a routine basis.
49
Special precautions should be taken to clean equipment
and compounding areas meticulously after preparing prod-
ucts that contain allergenic ingredients (e.g., sulfonamides
and penicillins). Equipment should be of appropriate design
and size for compounding and suitable for the intended uses.
Equipment and accessories used in compounding should be
inspected, maintained, and cleaned at appropriate intervals
to ensure the accuracy and reliability of their performance.
14
Computer entry, order processing, label generation, and
record keeping should be performed outside the critical area.
The controlled area should be well organized
50
and lighted
51
and of sufficient size to support sterile compounding activi-
ties. For hand washing, a sink with hot and cold running wa-
ter should be in close proximity to but outside the controlled
area. Refrigeration, freezing, ventilation, and room tempera-
ture control capabilities appropriate for storage of ingredients,
supplies, and pharmacy-prepared sterile products in accor-
dance with manufacturer, USP, and state or federal require-
ments should exist. The controlled area should be cleaned
and disinfected at regular intervals with appropriate agents,
according to written policies and procedures.
52
Disinfectants
should be alternated periodically to prevent development of
resistant microorganisms.
d
The floors of the controlled area
should be nonporous and washable to enable regular disinfec-
tion. Active work surfaces in the controlled area (e.g., carts,
compounding devices, counter surfaces) should be disin-
fected, in accordance with written procedures. Refrigerators,
freezers, shelves, and other areas where pharmacy-prepared
sterile products are stored should be kept clean.
Sterile products must be prepared in a class 100 envi-
ronment (i.e., the critical area).
29
Such an environment ex-
ists inside a certified horizontal- or vertical-laminar-airflow
workbench, a class 100 cleanroom, or a barrier isolator.
53
Cytotoxic and other hazardous products should be prepared
in a vented class II biological safety cabinet or a barrier isola-
tor of appropriate design to meet the personnel exposure lim-
its described in product material safety data sheets (MSDS).
54
Barrier isolators are gaining favor as clean environments, es-
pecially for cytotoxic drug compounding.
55–57
Properly main-
tained barrier isolators provide suitable environments for the
preparation of risk level 1, 2, and 3 sterile products.
58
Laminar-airflow workbenches are designed to be oper-
ated continuously. If a laminar-airflow workbench is turned
off between aseptic processes, it should be operated long
enough to allow complete purging of room air from the criti-
cal area (e.g., at least 30 minutes), then disinfected before use.
Barrier isolators, because of their closed nature, require less
start-up time. If the barrier isolator has been turned off for less
than 24 hours, a two-minute start-up time is sufficient. For
periods greater than 24 hours, the chamber should be sanitized
and the isolator should not be used for a minimum of 10 min-
utes after application of the sanitizing agent. The critical-area
work surface and all accessible interior surfaces of the work-
bench should be disinfected with an appropriate agent before
work begins and periodically thereafter, in accordance with
written policies and procedures.
52
The exterior surfaces of the
laminar-airflow workbench should be cleaned periodically
with a mild detergent or suitable disinfectant; 70% isopropyl
alcohol may damage the workbench’s clear plastic surfaces.
The laminar-airflow workbench should be certified by a quali-
fied contractor
59
every six months
53
or when it is relocated
to ensure operational efficiency and integrity. Prefilters in the
laminar-airflow workbench should be changed (or cleaned, if
they are washable) periodically (e.g., monthly), in accordance
with written policies and procedures.
A method should be established for calibrating and ver-
ifying the accuracy of automated compounding devices used
in aseptic processing (e.g., routine reconstitution of bulk or
individual vials, transferring of doses from a bulk container
to a minibag, syringe, or other single-dose container).
RL 1.5: Garb.
60
Procedures should require that personnel
wear clean gowns or coveralls that generate few particles
in the controlled area.
53
Scrub attire by itself is not accept-
able (but can, like street clothes, be covered by a gown or
coverall). Hand, finger, and wrist jewelry should be mini-
mized or eliminated. Fingernails should be kept clean and
trimmed. Head and facial hair should be covered. Masks
are recommended because most personnel talk
61
or may
cough or sneeze. Gloves are recommended. Personnel who
have demonstrated sensitivity to latex should use either
powder-free, low-latex protein gloves or, in the case of
severe allergy, latex-free (synthetic) gloves.
62,63

Drug Distribution and Control: Preparation and Handling–Guidelines 95
RL 1.6: Aseptic Technique
64,65
and Product Preparation.
66
Sterile products must be prepared with aseptic technique in
a class 100 environment. Personnel should scrub their hands
and forearms for an appropriate length of time with a suitable
antimicrobial skin cleanser at the beginning of each aseptic
compounding process and when reentering the controlled
area, in accordance with written procedures. Personnel
should wear appropriate attire (see RL 1.5: Garb). Eating,
drinking, and smoking are prohibited in the controlled area.
Talking should be minimized in the critical area during asep-
tic preparation (even when masks are worn).
Ingredients used to compound sterile products should
be determined to be stable, compatible, and appropriate for
the product to be prepared, according to manufacturer or USP
guidelines or appropriate scientific references. The ingredients
of the preparation should be predetermined to result in a final
product that meets physiological norms for solution osmolality
and pH, as appropriate for the intended route of administration.
Each ingredient and container should be inspected for defects,
expiration date, and product integrity before use. Expired, in-
appropriately stored, or defective products must not be used
in preparing sterile products. Defective products should be
promptly reported to the FDA MedWatch Program.
67
Only materials essential for preparing the sterile product
should be placed in the laminar-airflow workbench or barrier
isolator. The surfaces of ampuls, vials, and container closures
(e.g., vial stoppers) should be disinfected by swabbing or spray-
ing with an appropriate disinfectant solution (e.g., 70% isopro-
pyl alcohol or 70% ethanol) before placement in the work-
bench. Materials used in aseptic preparation should be arranged
in the critical area (within the laminar-airflow workbench or
barrier isolator) in a manner that prevents interruption of the
unidirectional airflow between the high-efficiency particulate
air (HEPA) filter and critical sites of needles, vials, ampuls,
containers, and transfer sets. All aseptic procedures should be
performed at least 6 inches inside the front edge of the laminar-
airflow workbench, in a clear path of unidirectional airflow
between the HEPA filter and work materials (e.g., needles, clo-
sures). The number of personnel preparing sterile products in
the workbench at one time should be minimized. Overcrowding
of the critical work area may interfere with unidirectional
airflow and increase the potential for compounding errors.
Likewise, the number of units being prepared in the workbench
at one time should allow unobstructed airflow over critical
areas. Automated compounding devices and other equipment
placed in or adjacent to the critical area should be cleaned, dis-
infected, and placed to avoid contamination or disruption of the
unidirectional airflow between the HEPA filter and sterile sur-
faces. Closed systems like barrier isolators require less stringent
placement of sterile units and equipment because the critical
area encompasses the entire work surface. Hand and arm move-
ments are not critical because the walls of the barrier isolator
provide protection from the outside environment.
50
Aseptic technique should be used to avoid touch con-
tamination of sterile needles, syringe parts (e.g., plunger,
syringe tip), and other critical sites. Solutions from ampuls
should be properly filtered to remove particles. Solutions of
reconstituted powders should be mixed carefully, ensuring
complete dissolution of the drug with the appropriate dilu-
ent. Needle entry into vials should be performed in such a
manner as to avoid coring of the vial closure. Some patients
may require a latex-free admixture to avoid severe allergic
reactions.
68
Latex-related policies and procedures should be
developed by each institution, given the paucity of evidence
that latex closures and syringe plungers are implicated in
patient reactions to latex.
69,70
Before, during, and after the
preparation of sterile products, the pharmacist should care-
fully check the identity and verify the amounts and sequence
of the additives in sterile preparations against the original pre-
scription, medication order, or other appropriate documenta-
tion (e.g., computerized patient profile, label generated from
a pharmacist-verified order) before the product is released or
dispensed.
RL 1.7: Process Validation.
71
Validation of aseptic pro-
cessing procedures provides a mechanism for ensuring that
processes consistently result in sterile products of accept-
able quality.
10
In risk level 1, process validation (or pro-
cess simulation) of compounding procedures is actually a
method of assessing the adequacy of an operator’s aseptic
technique. Each individual involved in the preparation of
sterile products should successfully complete a validation
process on technique before being allowed to prepare sterile
products. The validation process should follow written pro-
cedures.
42,43,45
Commercial kits are available for process val-
idation; however, their ability to support microbial growth
should be tested by challenging the intended kit with an in-
dicator organism (e.g., Bacillus stearothermophilus) that can
be purchased in known concentrations, is known not to be
pathogenic, and grows only at relatively high temperatures.
Process simulation allows for the evaluation of oppor-
tunities for microbial contamination during all steps of sterile
product preparation. The sterility of the final product is a cu-
mulative function of all processes involved in its preparation
and is ultimately determined by the processing step providing
the lowest probability of sterility.
31
Process simulation test-
ing is carried out in the same manner as normal production,
except that an appropriate microbiological growth medium is
used in place of the actual product used during sterile prepara-
tion. The same personnel, procedures, equipment, and materi-
als are involved. Completed medium samples are incubated.
If no microbial growth is detected, this provides evidence that
adequate aseptic technique was used. If growth is detected, the
entire sterile preparation process must be evaluated, corrective
action taken, and the process simulation test performed again.
No products intended for patient use should be prepared by
an individual until the process simulation test indicates that
the individual can competently perform aseptic procedures. It
is recommended that personnel competency be revalidated at
least annually, whenever the quality assurance program yields
an unacceptable result, and whenever unacceptable techniques
are observed; this revalidation should be documented.
RL 1.8: Expiration Dating.
72
All pharmacy-prepared ster-
ile products should bear an appropriate expiration date. The
expiration date assigned should be based on currently avail-
able drug stability information and sterility considerations.
Sources of drug stability information include references (e.g.,
AHFS Drug Information,
73
Extended Stability for Parenteral
Drugs,
74
Handbook on Injectable Drugs,
75
King Guide to
Parenteral Admixtures
76
), manufacturer recommendations,
and reliable, published research. When interpreting published
drug stability information, the pharmacist should consider all
aspects of the final sterile product being prepared (e.g., drug
reservoir, drug concentration, storage conditions). Methods
used for establishing expiration dates should be documented.

96 Drug Distribution and Control: Preparation and Handling–Guidelines
Appropriate inhouse (or contract service) stability testing may
be used to determine expiration dates when drug stability
data are not readily available. Home care pharmacies are of-
ten required to assign extended beyond-use dates to sterile
products, so ASHP has published guidelines for home care
pharmacies that address beyond-use dating.
74,77
RL 1.9: Labeling.
78
Sterile products should be labeled with
at least the following information:
1. For patient-specific products: the patient’ name and
any other appropriate patient identification (e.g.,
location, identification number); for batch-prepared
products: control or lot number,
2. All solution and ingredient names, amounts, strengths,
and concentrations (when applicable),
3. Expiration date and time, when applicable,
4. Prescribed administration regimen, when appropriate
(including rate and route of administration),
5. Appropriate auxiliary labeling (including precautions),
6. Storage requirements,
7. Identification (e.g., initials) of the responsible pharma-
cist (and technician),
8. Device-specific instructions (when appropriate), and
9. Any additional information, in accordance with state
or federal requirements; for example, a prescription
number for products dispensed to ambulatory care,
long-term-care, and home care patients.
The label should be legible and affixed to the final
container in a manner enabling it to be read while the ster-
ile product is being administered (when possible). Written
policies and procedures should address proper placement of
labels on containers.
79
RL 1.10: End-Product Evaluation.
80
The final product
should be inspected when preparation is completed and again
when the product is dispensed. This inspection includes an
evaluation for container leaks, container integrity, solution
cloudiness or phase separation, particulates in the solution,
appropriate solution color, and solution volume. The respon-
sible pharmacist should verify that the product was com-
pounded accurately with the correct ingredients, quantities of
each ingredient, containers, and reservoirs; different methods
may be used for end-product verification (e.g., observation,
calculation checks, documented records). Refractive index
measurement may also be used to verify the addition of
dextrose, for example in parenteral nutrient solutions.
81
RL 1.11: Handling of Sterile Products Outside the Phar-
macy.
82
Pharmacists should participate in developing proce-
dures for the safe use (e.g., stability, sterility) of sterile prod-
ucts once they are distributed outside the pharmacy. How the
product is transported from the pharmacy, how it is stored
outside the pharmacy, and methods for return, recycling, and
disposal should be addressed in written policies and proce-
dures.
15,83
Sterile products should be transported so as to be
protected from extremes of temperature outside their range
of stability and from light if they are photosensitive. Storage
containers and packaging verified as suitable for protection
during transport should be specified. Transit time and condi-
tions should also be specified and controlled. Delivery person-
nel should be instructed on special handling procedures. Once
delivered to the end user, sterile products should be appropri-
ately stored before use. Pharmacists should ascertain that the
user has appropriate locations and equipment for storage (e.g.,
a refrigerator with a suitable thermometer). Special instructions
for storage should be a part of the label or a separate information
sheet (e.g., instructions for cleanliness, proper storage, interpre-
tation of the expiration date and how to look for signs of product
deterioration). The pharmacist should be notified if storage con-
ditions do not remain suitable so that the pharmacist can give
advice as to the disposition of the sterile products and remedies
for storage problems. Pharmacists should participate in train-
ing end users on the proper care and storage of sterile products,
either directly or through written instructional materials.
RL 1.12: Documentation.
84
The following should be docu-
mented and maintained on file for an adequate period of
time, according to organizational policies and state regulatory
requirements: (1) the training and competency evaluation
of employees in sterile product procedures, (2) refrigerator
and freezer temperatures, (3) certification of laminar-airflow
workbenches, and (4) other facility quality control logs spe-
cific to the pharmacy’s policies and procedures (e.g., cleaning
logs for facilities and equipment). Pharmacists should also
maintain appropriate dispensing records for sterile products,
in accordance with state regulatory requirements.
Quality Assurance for Risk Level 2
Because the risks of inaccurate products are associated with
more complex procedures and because instability and con-
tamination are more likely with long-term storage and ad-
ministration, more stringent requirements are appropriate for
risk level 2 preparations. These requirements may be viewed
as more important in circumstances where the medical need
is routine. In circumstances where the medical need for a
product is immediate (and there is not a suitable alternative)
or when the preparation of such a product is rare, profes-
sional judgment should be applied to the extent to which
some guidelines (e.g., cleanroom design and final product
testing before product dispensing) must be applied.
RL 2.1: Policies and Procedures. In addition to all guide-
lines for risk level 1, a written quality assurance program
should define and identify necessary environmental monitoring
devices and techniques to be used to ensure an adequate envi-
ronment for risk level 2 sterile product preparation. Examples
include the use of airborne particle counters, air velocity and
temperature meters, viable particle samplers (e.g., slit samplers),
agar plates, and swab sampling of surfaces and potential con-
tamination sites. All aspects of risk level 2 sterile product prepa-
ration, storage, and distribution, including such details as the
choice of cleaning materials and disinfectants and the monitor-
ing of equipment accuracy, should be addressed in written poli-
cies and procedures. Limits of acceptability (threshold or action
levels) for environmental monitoring and process validation
and actions to be implemented when thresholds are exceeded
should be defined in written policies. For sterile batch com-
pounding, written policies and procedures should be established
for the use of master formulas and work sheets and for appropri-
ate documentation. Policies and procedures should also address
personnel attire in the controlled area, lot number determination
and documentation, and any other quality assurance procedures
unique to compounding risk level 2 sterile products.

Drug Distribution and Control: Preparation and Handling–Guidelines 97
RL 2.2: Personnel Education, Training, and Evaluation.
All guidelines for risk level 1 should be met. In addition to
guidelines for risk level 1, assessment of the competency
of personnel preparing risk level 2 sterile products should
include appropriate process validation (as described in RL
1.7: Process validation). However, process simulation pro-
cedures for assessing the preparation of risk level 2 sterile
products should be representative of all types of manipu-
lations, products, and batch sizes personnel preparing risk
level 2 products are likely to encounter.
15
Personnel should
also be taught which products are to undergo end-product
quantitative analysis (see RL 2.10).
RL 2.3: Storage and Handling. All storage and handling
guidelines for risk level 1 should be met.
RL 2.4: Facilities and Equipment. In addition to all guide-
lines for risk level 1, the following guidelines should be fol-
lowed for risk level 2 sterile product preparation:
1. The controlled area should meet the standards of a class
10,000 cleanroom,
e
as defined by Federal Standard
209E.
85,f
A positive air pressure relative to adjacent
pharmacy areas is required, as are an appropriate num-
ber of air exchanges per hour and appropriate humidity
and temperature levels.
86
For open-architecture clean-
rooms, it is appropriate to measure the volume of air
entering the cleanroom versus the volume of air enter-
ing adjacent rooms, so as to ensure a positive pressure
gradient for the cleanroom. To allow proper cleaning
and disinfection, walls, floors, and ceilings in the con-
trolled area should be nonporous. To help reduce the
number of particles in the controlled area, an adjacent
support area (e.g., ante-room) should be provided. A
properly maintained barrier isolator also provides an
acceptable environment.
57
A barrier isolator provides a
class 100 environment for product preparation; there-
fore, the isolator itself can be in a separate area of the
pharmacy but need not actually be in a cleanroom.
2. Cleaning materials (e.g., mops, sponges, and germicidal
disinfectants) for use in the cleanroom should be carefully
selected. They should be made of materials that generate
a low amount of particles. If reused, cleaning materials
should be cleaned and disinfected between uses.
3. The critical-area work surfaces (e.g., interior of the
laminar-airflow workbench) should be disinfected fre-
quently and before and after each batch-preparation
process with an appropriate agent, according to written
policies and procedures. Floors should be disinfected at
least daily. Carpet or porous floors, porous walls, and
porous ceiling tiles are not suitable in the controlled area
because these surfaces cannot be properly cleaned and
disinfected. Exterior workbench surfaces and other hard
surfaces in the controlled area, such as shelves, carts,
tables, and stools, should be disinfected weekly and after
any unanticipated event that could increase the risk of
contamination. Walls should be cleaned at least monthly.
4. To ensure that an appropriate environment is maintained
for risk level 2 sterile product preparation, an effective
written environmental monitoring program is recom-
mended.
87
Sampling of air and surfaces according to a
written plan and schedule is recommended.
31
The plan
and frequency should be adequate to document that the
controlled area is suitable and that the laminar-airflow
workbench or biological safety cabinet meets class 100
requirements. Limits of acceptability (thresholds or
action levels) and appropriate actions to be taken in
the event thresholds are exceeded should be specified.
USP presents examples of environmental monitoring.
15
Settle plates or wipe samples can provide a simple but
effective means of routinely monitoring airborne micro-
bial contamination in controlled and critical areas.
45,88,89
5. To help reduce the number of particles in the controlled
area, an adjacent support area (e.g., anteroom) of high
cleanliness, separated from the controlled area by a bar-
rier (e.g., plastic curtain, partition, wall), is recommended.
Appropriate activities for the support area include, but
are not limited to, hand washing, gowning and gloving,
removal of packaging and cardboard items, and cleaning
and disinfecting hard-surface containers and supplies be-
fore placing these items into the controlled area.
6. Methods should be established for calibrating and
verifying the accuracy and sterility of automated com-
pounding methods used in aseptic processing.
90–96
RL 2.5: Garb. All guidelines for risk level 1 should be met.
Gloves, gowns, and masks are required for the preparation of
all risk level 2 sterile products. Even when sterile gloves are
used, they do not remain sterile during aseptic compound-
ing; however, they do assist in containing bacteria, skin, and
other particles that may be shed even from scrubbed hands.
Clean gowns, coveralls, or closed jackets with sleeves hav-
ing elastic binding at the cuff are recommended; these gar-
ments should be made of low-shedding materials. Shoe
covers may be helpful in maintaining the cleanliness of the
controlled area. Barrier isolators do not require the same
level of gowning as laminar-airflow workstations as long as
they operate as closed systems with HEPA filtration of air
entering and leaving the barrier isolator and a separate area
for entrance, such as an air lock for product transfers.
During sterile product preparation, gloves should be
rinsed frequently with a suitable agent (e.g., 70% isopropyl
alcohol) and changed when their integrity is compromised
(i.e., when they are punctured or torn). Personnel should dis-
card gloves upon leaving the cleanroom and don new gloves
upon reentering the cleanroom.
RL 2.6: Aseptic Technique and Product Preparation.
97–99
All
guidelines for risk level 1 sterile product preparation should be
met. Relative to batch-prepared products, a master work sheet
should be developed for a batch of each discrete identity and
concentration of sterile product to be prepared. The master
work sheet should consist of the formula, components, com-
pounding directions or procedures, a sample label, and evalu-
ation and testing requirements. Once the original master work
sheet is approved by the designated pharmacist, a verified du-
plicate (e.g., a photocopy) of the master work sheet should be
used as the preparation work sheet from which each batch is
prepared and on which all documentation for each batch oc-
curs. (For small-formula, frequently prepared batches, it may
be more efficient to have multiple lines on the preparation work
sheet for documenting more than one batch.) The preparation
work sheet should be used to document the following:
1. Identity of all solutions and ingredients and their cor-
responding amounts, concentrations, or volumes,

98 Drug Distribution and Control: Preparation and Handling–Guidelines
2. Manufacturer lot number and expiration date for each
component,
3. Component manufacturer or suitable manufacturer
identification number,
4. Container specifications (e.g., syringe, pump cassette),
5. Lot or control number assigned to batch,
6. Expiration date of batch-prepared products,
7. Date of preparation,
8. Identity (e.g., initials, codes, signatures) of personnel
involved in preparation,
9. End-product evaluation and testing specifications and
results,
10. Storage requirements,
11. Specific equipment used during aseptic preparation
(e.g., a specific automated compounding device), and
12. Comparison of actual yield with anticipated yield,
when appropriate.
However documentation is done, a procedure should
exist for easy retrieval of all records pertaining to a particu-
lar batch. Each batch of sterile products should bear a unique
lot number. Identical lot numbers must never be assigned to
different products or different batches of the same product.
Lot numbers may be alphabetic, numeric, or alphanumeric.
The process of combining multiple sterile ingredients
into a single sterile reservoir for subdivision into multiple
units for dispensing may necessitate additional quality
control procedures. A second pharmacist should verify
calculations associated with this process, when possible;
this verification should be documented. Because this process
often involves making multiple entries into the intermediate
sterile reservoir, the likelihood of contamination may be
greater than that associated with the preparation of other risk
level 2 sterile products.
For preparation involving automated compounding de-
vices, a pharmacist should verify data entered into the com-
pounding device before compounding begins. End-product
checks should be performed to verify accuracy of ingredient
delivery. These checks may include weighing and visually
verifying the final product. For example, the expected weight
(in grams) of the final product, based on the specific gravi-
ties of the ingredients and their respective volumes, can be
documented on the compounding formula sheet, dated, and
initialed by the responsible pharmacist. Once compounding is
completed, each final product can be weighed and its weight
compared with the expected weight. The product’s actual
weight should fall within a preestablished threshold for vari-
ance. Visual verification may be aided by marking the begin-
ning level of each bulk container before starting the automated
mixing process and checking each container after completing
the mixing process to determine whether the final levels ap-
pear reasonable in comparison with expected volumes. The
operator should also periodically observe the device during
the mixing process to ensure that the device is operating prop-
erly (e.g., check to see that all stations are operating). If there
are doubts whether a product or component has been properly
prepared or stored, the product should not be used.
RL 2.7: Process Validation. Each individual involved in the
preparation of risk level 2 sterile products should success-
fully complete a validation process, as recommended for
risk level 1. Process simulation for compounding risk level
2 sterile products should be representative of all types of
manipulations, products, and batch sizes that personnel pre-
paring risk level 2 sterile products are likely to encounter.
RL 2.8: Expiration Dating. All guidelines for risk level 1
should be met.
RL 2.9: Labeling. All guidelines for risk level 1 should be met.
RL 2.10: End-Product Evaluation. All guidelines for risk
level 1 should be met. For complex or toxic products, it is
appropriate, when possible, to obtain quantitative testing of
the accuracy of sterile additives, for example, the dextrose
concentration in pediatric parenteral nutrient solutions or the
potassium concentration in cardioplegia solutions.
g
RL 2.11: Handling of Sterile Products Outside the Phar-
macy. All guidelines for risk level 1 should be met.
RL 2.12: Documentation. All guidelines for risk level 1
should be met. Additionally, documentation of end-product
sampling and batch-preparation records should be main-
tained for an adequate period, in accordance with organiza-
tional policies and procedures and state regulatory require-
ments.
100
Documentation for sterile batch-prepared products
should include the
1. Master work sheet,
2. Preparation work sheet, and
3. End-product evaluation and testing results.
Quality Assurance for Risk Level 3
Risk level 3 addresses the preparation of products that pose the
greatest potential risk to patients. The quality assurance activi-
ties described in this section are clearly more demanding—in
terms of processes, facilities, and final product assessment—
than for risk levels 1 and 2. Ideally, the activities described for
risk level 3 would be used for all high-risk products. However,
the activities may be viewed as most important in circum-
stances where the medical need for such high-risk products is
routine. In circumstances where the medical need for such a
product is immediate (and there is not a suitable alternative)
or when the preparation of such a product is rare, professional
judgment must be applied as to the extent to which some ac-
tivities (e.g., strict facility design, quarantine, and final product
testing before product dispensing) should be applied.
RL 3.1: Policies and Procedures. There should be written
policies and procedures related to every aspect of preparation
of risk level 3 sterile products. These policies and procedures
should be detailed enough to ensure that all products have the
identity, strength, quality, and purity purported for the prod-
uct.
14,101
All policies and procedures should be reviewed and
approved by the designated pharmacist. There should be a
mechanism designed to ensure that policies and procedures
are communicated, understood, and adhered to by personnel
cleaning or working in the controlled area or support area.
Written policies and procedures should define and identify the
environmental monitoring activities necessary to ensure an ad-
equate environment for risk level 3 sterile product preparation.
In addition to the policies and procedures required for
risk levels 1 and 2, there should be written policies and pro-
cedures for the following:

Drug Distribution and Control: Preparation and Handling–Guidelines 99
1. Component selection, handling, and storage,
2. Any additional personnel qualifications commensurate
with the preparation of risk level 3 sterile products,
3. Personnel responsibilities in the controlled area (e.g., steril-
ization, cleaning, maintenance, access to controlled area),
4. Equipment use, maintenance, calibration, and testing,
5. Sterilization and expiration dating,
6. Master formula and master work sheet development
and use,
7. End-product evaluation and testing,
8. Appropriate documentation for preparation of risk
level 3 sterile products,
9. Use, control, and monitoring of environmentally con-
trolled areas and calibration of monitoring equipment,
10. Process simulation for each risk level 3 sterile product,
11. Quarantine of products and release from quarantine,
if applicable,
12. A mechanism for recalling products from patients in
the event that end-product testing procedures yield un-
acceptable results, and
13. Any other quality control procedures unique to the
preparation of risk level 3 sterile products.
RL 3.2: Personnel Education, Training, and Evaluation.
Persons preparing sterile products at risk level 3 must have
specific education, training, and experience to perform all
functions required for the preparation of risk level 3 ster-
ile products. However, final responsibility should lie with
the pharmacist, who should be knowledgeable in pharmacy
compounding practice
14
and proficient in quality assurance
requirements, equipment used in the preparation of risk
level 3 sterile products, and other aspects of sterile product
preparation. The pharmacist should have sufficient educa-
tion, training, experience, and demonstrated competency to
ensure that all sterile products prepared from sterile or non-
sterile components have the identity, strength, quality, and
purity purported for the products.
101
In addition to the body
of knowledge required for risk levels 1 and 2, the pharmacist
should possess sufficient knowledge in the following areas:
1. Aseptic processing,
2. Quality control and quality assurance as related to
environmental, component, and end-product testing,
3. Sterilization techniques,
98
and
4. Container, equipment, and closure system selection.
All pharmacy personnel involved in the cleaning
and maintenance of the controlled area should be specially
trained and thoroughly knowledgeable in the special re-
quirements of class 100 critical-area technology and design.
There should be documented, ongoing training for all em-
ployees to enable retention of expertise.
RL 3.3: Storage and Handling. In addition to guidelines for risk
levels 1 and 2, risk level 3 policies and procedures for storage
and handling should include procurement, identification, stor-
age, handling, testing, and recall of nonsterile components.
14,101
Components and finished products ready to undergo
end-product testing should be stored in a manner that pre-
vents their use before release by a pharmacist, minimizes
the risk of contamination, and enables identification. There
should be identified storage areas that can be used to quaran-
tine products, if necessary, before they are released.
15
RL 3.4: Facilities and Equipment. Preparation of risk level
3 sterile products should occur in a class 100 horizontal- or
vertical-laminar-airflow workbench that is properly situated
in a class 10,000 cleanroom or in a properly maintained and
monitored class 100 cleanroom (without the workbench).
102
The cleanroom area should have a positive pressure differen-
tial relative to adjacent, less clean areas of at least 0.05 inch
of water. A properly designed and maintained barrier isolator
provides an aseptic environment for risk level 3 products.
To allow proper cleaning and disinfection, walls, floors,
and ceilings in the controlled area should be nonporous. To
help reduce the number of particles in the controlled area, an
adjacent support area (e.g., anteroom) should be provided.
During the preparation of risk level 3 sterile products,
access to the controlled area or cleanroom should be limited
to those individuals who are required to be in the area and
are properly attired. The environment of the main access ar-
eas directly adjacent to the controlled area (e.g., anteroom)
should meet at least Federal Standard 209E class 100,000
requirements. To help maintain a class 100 critical-area en-
vironment during compounding, the adjacent support area
(e.g., anteroom) should be separated from the controlled area
by a barrier (e.g., plastic curtain, partition, wall). Written
policies and procedures for monitoring the environment of
the controlled area and adjacent areas should be developed.
No sterile products should be prepared in the con-
trolled area if it fails to meet established criteria specified
in the policies and procedures. A calibrated particle counter
capable of measuring air particles 0.5 mm and larger should
be used to monitor airborne particulate matter.
103
Before
product preparation begins, the positive-pressure air status
should meet or exceed the requirements. Air samples should
be taken at several places in the controlled area with the ap-
propriate environmental monitoring devices (e.g., nutrient
agar plates). Surfaces on which work actually occurs, in-
cluding laminar-airflow workbench surfaces and tabletops,
should be monitored by using surface contact plates, the
swab-rinse technique, or other appropriate methods.
104
Test results should be reviewed and criteria should be
pre established to determine the point at which the preparation
of risk level 3 sterile products will be disallowed until correc-
tive measures are taken. When the environment does not meet
the criteria specified in the policies and procedures, sterile prod-
uct processing should immediately cease and corrective action
should be taken. In the event that this occurs, written policies and
proce dures should delineate alternative methods of sterile prod-
uct preparation to enable timely fulfillment of prescription orders.
Equipment should be adequate to prevent microbio-
logical contamination. Methods should be established for
the cleaning, preparation, sterilization, calibration, and doc-
umented use of all equipment.
Critical-area work surfaces should be disinfected with
an appropriate agent before the preparation of each product.
Floors in the controlled area should be disinfected at least daily.
Exterior workbench surfaces and other hard surfaces in the
controlled area, such as shelves, tables, and stools, should be
disinfected weekly and after any unanticipated event that could
increase the risk of contamination. Walls and ceilings in the con-
trolled area or cleanroom should be disinfected at least weekly.
Large pieces of equipment, such as tanks, carts, and
tables, used in the controlled area or cleanroom should be made
of a material that can be easily cleaned and disinfected; stainless
steel is recommended. Stools and chairs should be cleanroom

100 Drug Distribution and Control: Preparation and Handling–Guidelines
quality. Equipment that does not come in direct contact with
the finished product should be properly cleaned, rinsed, and
disinfected before being placed in the controlled area. All non-
sterile equipment that will come in contact with the sterilized
final product should be properly sterilized before introduction
into the controlled area; this precaution includes such items as
tubing, filters, containers, and other processing equipment. The
sterilization process should be monitored and documented.
101
RL 3.5: Garb. All guidelines for risk levels 1 and 2 should
be met. Additionally, cleanroom garb should be worn inside
the controlled area at all times during the preparation of
risk level 3 sterile products. Attire should consist of a low-
shedding coverall, head cover, face mask, and shoe covers.
These garments may be either disposable or reusable. Head
and facial hair should be covered. Before donning these
garments over street clothes, personnel should thoroughly
wash their hands and forearms with a suitable antimicrobial
skin cleanser.
25
Sterile disposable gloves should be worn
and rinsed frequently with an appropriate agent (e.g., 70%
isopropyl alcohol) during processing. The gloves should be
changed if their integrity is compromised. If persons leave
the controlled area or support area during processing, they
should regown with clean garments before reentering.
RL 3.6: Aseptic Technique and Product Preparation. All
guidelines for risk levels 1 and 2 should be met. Methods
should ensure that components and containers remain free
from contamination and are easily identified as to the prod-
uct, lot number, and expiration date. If components are not
finished sterile pharmaceuticals obtained from licensed
manufacturers, pharmacists should ensure that these compo-
nents meet USP and FDA standards. Products prepared from
nonsterile ingredients should be tested to ensure that they do
not exceed specified endotoxin limits, unless the ingredient
will denature all proteins (e.g., concentrated hydrochloric
acid).
105
As each new lot of components and containers is
received, the components should be quarantined until prop-
erly identified, tested, or verified by a pharmacist.
101
The methods for preparing sterile products and using
process controls should be designed to ensure that finished
products have the identity, strength, quality, and purity they
are intended to have. Any deviations from established meth-
ods should be documented and appropriately justified.
A master work sheet should be developed for the prep-
aration of each risk level 3 sterile product. Once the phar-
macist approves the master work sheet, a verified duplicate
of the master work sheet should be used as the controlling
document from which each sterile end product or batch of
prepared products is compounded and on which all docu-
mentation for that product or batch occurs. The preparation
work sheet should document all the requirements for risk
level 2 plus the following:
1. Comparison of actual with anticipated yield,
2. Sterilization methods,
106,107
3. Pyrogen testing,
108
and
4. Quarantine specifications.
The preparation work sheet should serve as the batch
record for each time a risk level 3 sterile product is prepared.
Each batch of pharmacy-prepared sterile products should
bear a unique lot number, as described in risk level 2.
There should be documentation on the preparation
work sheet of all additions of individual components plus
the signatures or initials of those individuals involved in the
measuring or weighing and addition of these components.
The selection of the final packaging system (including
container and closure) for the sterile product is crucial to main-
taining product integrity.
109
To the extent possible, presterilized
containers obtained from licensed manufacturers should be
used. If an aseptic filling operation is used, the container should
be sterile at the time of the filling operation. If nonsterile con-
tainers are used, methods for sterilizing these containers should
be established. Final containers selected should be capable of
maintaining product integrity (i.e., identity, strength, quality,
and purity) throughout the shelf life of the product.
110
For products requiring sterilization, selection of an
appropriate method of sterilization is of prime importance.
Methods of product sterilization include sterile filtration,
auto claving, dry heat sterilization, chemical sterilization, and
irra diation.
111,112
The pharmacist must ensure that the steriliza-
tion method used is appropriate for the product components
and does not alter the pharmaceutical properties of the final
product. A method of sterilization often used by pharmacists
is sterile filtration.
113
In sterile filtration, the filter should
be chosen to fit the chemical nature of the product, and the
product should be filtered into presterilized containers under
aseptic conditions. Sterilizing filters of 0.22-μm or smaller
porosity should be used in this process. Colloidal or viscous
products may require a 0.45-μm filter; however, extreme cau-
tion should be exercised in these circumstances, and more
stringent end-product sterility testing is essential.
114
To ensure that a bacteria-retentive filter did not rup-
ture during filtration of a product, an integrity test should be
performed on all filters immediately after filtration. This test
may be accomplished by performing a bubble point test, in
which pressurized gas (e.g., air in a syringe attached to the
used filter) is applied to the upstream side of the filter with
the downstream outlet immersed in water and the pressure at
which a steady stream of bubbles begins to appear is noted.
98
The observed pressure is then compared with the manufac-
turer’s specification for the filter. To compare the used fil-
ter with the manufacturer’s specifications, which would be
based on the filtration of water through the filter, it is neces-
sary to first rinse the filter with sterile water for injection. An
observed value lower than the manufacturer’s specification
indicates that the filter was defective or ruptured during the
sterilization process. Methods should be established for han-
dling, testing, and resterilizing any product processed with a
filter that fails the integrity test.
RL 3.7: Process Validation. In addition to risk level 1 and 2
guidelines, written policies and procedures should be estab-
lished to validate all processes involved in the preparation of
risk level 3 sterile products (including all procedures, equip-
ment, and techniques) from sterile or nonsterile components.
In addition to evaluating personnel technique, process vali-
dation provides a mechanism for determining whether a par-
ticular process will, when performed by qualified personnel,
consistently produce the intended results.
115
RL 3.8: Expiration Dating. In addition to risk level 2 guide-
lines, there should be reliable methods for establishing all
expiration dates, including laboratory testing of products
for sterility, nonpyrogenicity, and chemical content, when

Drug Distribution and Control: Preparation and Handling–Guidelines 101
necessary. These tests should be conducted in a manner based
on appropriate statistical criteria, and the results documented.
RL 3.9: Labeling. All guidelines for risk levels 1 and 2
should be met.
RL 3.10: End-Product Evaluation. For each preparation of
a sterile product or a batch of sterile products, there should
be appropriate laboratory determination of conformity (i.e.,
purity, accuracy, sterility, and nonpyrogenicity) to estab-
lished written specifications and policies. Any reprocessed
material should undergo complete final product testing.
Additionally, process validation should be supplemented
with a program of end-product sterility testing, according to
a formal sampling plan.
116–127
Written policies and proce-
dures should specify measurements and methods of testing.
Policies and procedures should include a statistically valid
sampling plan and acceptance criteria for the sampling and
testing. The criteria should be statistically adequate to rea-
sonably ensure that the entire batch meets all specifications.
Products not meeting all specifications should be rejected
and discarded. There should be a mechanism for recalling
all products of a specific batch if end-product-testing pro-
cedures yield unacceptable results. On completion of final
testing, products should be stored in a manner that ensures
their identity, strength, quality, and purity.
It is advisable to quarantine sterile products com-
pounded from nonsterile components, pending the results
of end-product testing. If products prepared from nonsterile
components must be dispensed before satisfactory comple-
tion of end-product testing, there must be a procedure to
allow for immediate recall of the products from patients
to whom they were dispensed.
RL 3.11: Handling of Sterile Products Outside the Phar-
macy. All guidelines for risk levels 1 and 2 should be met.
RL 3.12: Documentation. In addition to the guidelines for
risk levels 1 and 2, documentation for risk level 3 sterile
products should include
1. Preparation work sheet,
2. Sterilization records of final products (if applicable),
3. Quarantine records (if applicable), and
4. End-product evaluation and testing results.
References
1. Hughes CF, Grant AF, Lick BD, et al. Cardioplegic
solution: a contamination crisis. J Thorac Cardiovasc
Surg. 1986; 91:296–302.
2. Pittsburgh woman loses eye to tainted drugs; 12 hurt.
Baltimore Sun. 1990; Nov 9:3A.
3. ASHP gears up multistep action plan regarding sterile
drug products. Am J Hosp Pharm. 1991; 48:386–90.
4. Dugleaux G, Coutour XL, Hecquard C, et al.
Septicemia caused by contaminated parenteral nutri-
tion pouches: the refrigerator as an unusual cause.
JPEN J Parenter Enteral Nutr. 1991; 15:474–5.
5. Solomon SL, Khabbaz RF, Parker RH, et al. An out-
break of Candida parapsilosis bloodstream infections
in patients receiving parenteral nutrition. J Infect Dis.
1984; 149:98–102.
6. Food and Drug Administration. Hazards of precipi-
tation with parenteral nutrition. Am J Hosp Pharm.
1994; 51:427–8.
7. Pierce LR, Gaines A, Varricchio R, et al. Hemolysis
and renal failure associated with use of sterile water
for injection to dilute 25% human albumin solution.
Am J Health-Syst Pharm. 1998; 55:1057,1062,1070.
8. Flynn EA, Pearson RE, Barker KN. Observational study
of accuracy in compounding i.v. admixtures at five hos-
pitals. Am J Health-Syst Pharm. 1997; 54:904–12.
9. Santell JP, Kamalich RF. National survey of quality as-
surance activities for pharmacy-prepared sterile prod-
ucts in hospitals and home infusion facilities—1995.
Am J Health-Syst Pharm. 1996; 53:2591–605.
10. Kastango ES, Douglass K. Improving the manage-
ment, operations and cost effectiveness of sterile-prod-
uct compounding. Int J Pharm Compd. 1999; 3:253–8.
11. Guynn JB Jr, Poretz DM, Duma RJ. Growth of various
bacteria in a variety of intravenous fluids. Am J Hosp
Pharm. 1973; 30:321–5.
12. Hasegawa GR. Caring about stability and compati-
bility. Am J Hosp Pharm. 1994; 51:1533–4. Editorial.
13. Stability considerations in dispensing practice (general
information chapter 1191). In: The United States phar-
macopeia, 24th rev., and The national formulary, 19th ed.
Rockville, MD: The United States Pharmacopeial
Convention; 1999:2128–30.
14. Pharmacy compounding practices (general information
chapter 1161). In: The United States pharmacopeia,
24th rev., and The national formulary, 19th ed.
Rockville, MD: The United States Pharmacopeial
Convention; 1999:2118–22.
15. Sterile drug products for home use (general informa-
tion chapter 1206). In: The United States pharmaco-
peia, 24th rev., and The national formulary, 19th ed.
Rockville, MD: The United States Pharmacopeial
Convention; 1999:2130–43.
16. Good compounding practices applicable to state
licensed pharmacies. Natl Pharm Compliance News.
1993; May:2–3, Oct:2–3.
17. Model rules for sterile pharmaceuticals. Chicago: National
Association of Boards of Pharmacy; 1993:12.1–3.
18. National Advisory Group on Standards and Practice
Guidelines for Parenteral Nutrition. Safe practices for
parenteral nutrition formulations. JPEN J Parenter
Enteral Nutr. 1998; 22:49–66.
19. Standard 3.3. Policies and procedures support safe
medication prescription or ordering. In: 1999 Hospital
accreditation standards. Chicago: Joint Commission on
Accreditation of Healthcare Organizations; 1999:88.
20. Standard TX 5.1. Medications are prepared safely.
In: 1999–2000 Comprehensive accreditation man-
ual for home care. Chicago: Joint Commission on
Accreditation of Healthcare Organizations; 1999:182.
21. Standard TX 2.3. The pharmacy organization maintains
proper conditions of sanitation, temperature, light, mois-
ture, ventilation, segregation, safety, and security for
preparing medications. 1996–1998 Standards for long
term care pharmacies. Chicago: Joint Commission on
Accreditation of Healthcare Organizations; 1996:70–1.
22. Standard TX 3.3. Prescribing and ordering of medi-
cations follow established procedures. 1998–99
Comprehensive accreditation manual for ambulatory

102 Drug Distribution and Control: Preparation and Handling–Guidelines
care. Chicago: Joint Commission on Accreditation of
Healthcare Organizations; 1998:211.
23. Food and Drug Modernization Act of 1997, Pub. L.
No. 105–115, 111 Stat. 2296.
24. Centers for Disease Control. Guideline for prevention
of intravascular infections. Am J Infect Control. 1983;
11(5):183–93.
25. Centers for Disease Control. Guideline for handwash-
ing and hospital environmental control. Am J Infect
Control. 1986; 4(8):110–29.
26. American Society of Hospital Pharmacists. ASHP tech-
nical assistance bulletin on handling cytotoxic and haz-
ardous drugs. Am J Hosp Pharm. 1990; 47:1033–49.
27. American Society of Hospital Pharmacists. ASHP tech-
nical assistance bulletin on pharmacy-prepared ophthal-
mic products. Am J Hosp Pharm. 1993; 50:1462–3.
28. Cleanrooms and associated controlled environments—
part 1: classification of air cleanliness. International
standard ISO 14644-1. 1st ed. New York: American
National Standards Institute; 1999.
29. Federal standard no. 209E. Airborne particulate cleanli-
ness classes in cleanrooms and clean zones. Washington,
DC: General Services Administration; 1992.
30. Microbiological evaluation of clean rooms and other con-
trolled environments (general information chapter 1116).
In: The United States Pharmacopeia, 24th rev., and The
national formulary, 19th ed. Rockville, MD: The United
States Pharmacopeial Convention; 1999:2009–106.
31. Validation of aseptic filling for solution drug products.
Technical monograph no. 22. Philadelphia: Parenteral
Drug Association; 1996.
32. Formulations: Int J Pharm Compd. 1999; 2:297–307.
33. Buchanan EC. Policies and procedures for sterile
product preparation. In: Principles of sterile prod-
uct preparation. Bethesda, MD: American Society of
Health-System Pharmacists; 1995:133–8.
34. Standard operating procedure of a horizontal laminar air
flow hood. Int J Pharm Compd. 1997(Sep/Oct); 1:344–5.
35. Standard operating procedure for general aseptic pro-
cedures carried out at a laminar air flow workbench.
Int J Pharm Compd. 1998(May/Jun); 2:242.
36. Standard operating procedure for particulate testing
for sterile products. Int J Pharm Compd. 1997(Jan/
Feb); 2:78.
37. Quality assurance of pharmacy-prepared sterile prod-
ucts. Bethesda, MD: American Society of Hospital
Pharmacists; 1994. Videotape and workbook.
38. Safe handling of cytotoxic and hazardous drugs.
Bethesda, MD: American Society of Health-System
Pharmacists; 1990. Videotape and study guide.
39. Schneider PJ, Buchanan EC. Personnel education,
training and evaluation. In: Principles of sterile prod-
uct preparation. Bethesda, MD: American Society of
Health-System Pharmacists; 1995:9–15.
40. Hunt ML. Training manual for intravenous admixture
personnel. 5th ed. Chicago: Precept; 1995.
41. Gallagher M. Home care pharmacist competency as-
sessment program. Am J Health-Syst Pharm. 1999;
56:1549–53.
42. Dirks I, Smith FM, Furtado D, et al. Method for testing
aseptic technique of intravenous admixture personnel.
Am J Hosp Pharm. 1982; 39:457–9.
43. Brier KL. Evaluating aseptic technique of pharmacy
personnel. Am J Hosp Pharm. 1983; 40:400–3.
44. McKinnon BT. Handling of sterile products within the
pharmacy. In: Principles of sterile product preparation.
Bethesda, MD: American Society of Health-System
Pharmacists; 1995:111–6.
45. Morris BG, Avis KE. Quality-control plan for intra-
venous admixture programs. 1: Visual inspection of
solutions and environmental testing. Am J Hosp
Pharm. 1980; 37:189–95.
46. Buchanan EC. Sterile compounding facilities. In:
Principles of sterile product preparation. Bethesda,
MD: American Society of Health-System Pharmacists;
1995:25–35.
47. Schneider PJ. Equipment for sterile product prepa-
ration. In: Principles of sterile product preparation.
Bethesda, MD: American Society of Health-System
Pharmacists; 1995:37–43.
48. Lau D, Shane R, Yen J. Quality assurance for sterile
products: simple changes can help. Am J Hosp Pharm.
1994; 51:1353. Letter.
49. Rahe H. Containment Technologies Group, Inc.
Personal communication. 1999 Oct.
50. Hunt ML. Training manual for intravenous admixture
personnel. 5th ed. Chicago: Precept; 1995:67–70.
51. Buchanan TL, Barker KN, Gibson JT, et al.
Illumination and errors in dispensing. Am J Hosp
Pharm. 1991; 48:2137–45.
52. Denny VF, Kopis EM, Marsik FJ. Elements for a suc-
cessful disinfection program in the pharmaceutical en-
vironment. PDA J Pharm Sci Technol. 1999; 53:115–24.
53. Frieben WR. Control of the aseptic processing envi-
ronment. Am J Hosp Pharm. 1983; 40:1928–35.
54. Scheckelhoff DJ. Handling, preparation and disposal
of cytotoxic and hazardous agents. In: Principles of
sterile product preparation. Bethesda, MD: American
Society of Health-System Pharmacists; 1995:63–9.
55. Favier M, Hansel S, Bressole F. Preparing cytotoxic
agents in an isolator. Am J Hosp Pharm. 1993; 50: 2335–9.
56. Mosko P, Rahe H. Barrier isolation technology: a
labor-efficient alternative to cleanrooms. Hosp Pharm.
1999; 34:834–8.
57. Pilong A, Moore M. Conversion to isolators in a
sterile preparation area. Am J Health-Syst Pharm.
1999; 56:1978–80.
58. Tillett L. Barrier isolators as an alternative to a clean-
room. Am J Health-Syst Pharm. 1999; 56:1433–6.
59. Bryan D, Marback RC. Laminar air flow equipment
certification: what the pharmacist needs to know. Am J
Hosp Pharm. 1984; 41:1343–9.
60. McKinnon BT. Personnel behavior and garb use. In:
Principles of sterile product preparation. Bethesda,
MD: American Society of Health-System Pharmacists;
1995:57–62.
61. Coriell LL, McGarrity GJ, Horneff J. Medical appli-
cations of dust-free rooms: I. Elimination of airborne
bacteria in a research laboratory. Am J Public Health.
1967; 57:1824–36.
62. NIOSH recommends steps for reducing work-related
exposure to latex. Am J Health-Syst Pharm. 1997;
54:1688,1691.
63. Dasher G, Dasher T. The growing problem of latex al-
lergies. Infusion. 1996; 2(Jan):23–7.
64. Hunt ML. Techniques used in preparing intravenous
admixtures. In: Training manual for intravenous ad-
mixture personnel. Chicago: Precept; 1995:87–103.

Drug Distribution and Control: Preparation and Handling–Guidelines 103
65. Scheckelhoff DJ. Use of aseptic technique. In:
Principles of sterile product preparation. Bethesda,
MD: American Society of Health-System Pharmacists;
1995:49–56.
66. Buchanan EC. Sterile product formulation and com-
pounding. In: Principles of sterile product preparation.
Bethesda, MD: American Society of Health-System
Pharmacists; 1995:17–24.
67. Kessler DA. MedWatch: The new FDA medical prod-
ucts reporting program. Am J Hosp Pharm. 1993;
50:1921–36.
68. Rice SP, Gutfeld MB. Preparation of latex-safe prod-
ucts. Am J Health-Syst Pharm. 1998; 55:1462–7.
69. Holzman RS. Latex allergy: an emerging operating
room problem. Anesth Analg. 1993; 76:635–41.
70. McDermott JS, Gura KM. Procedures for preparing
injectable medications for latex-sensitive patients. Am
J Health-Syst Pharm. 1997; 54:2516–7.
71. Schneider PJ. Process validation. In: Principles of
sterile product preparation. Bethesda, MD: American
Society of Health-System Pharmacists; 1995:121–4.
72. McKinnon BT. Factors influencing expiration dates.
In: Principles of sterile product preparation. Bethesda,
MD: American Society of Health-System Pharmacists;
1995:95–103.
73. McEvoy GK, ed. AHFS drug information 99.
Bethesda, MD: American Society of Health-System
Pharmacists; 1999.
74. Bing C, ed. Extended stability for parenteral drugs.
Bethesda, MD: American Society of Health-System
Pharmacists; in press.
75. Trissel LA. Handbook on injectable drugs. 10th ed.
Bethesda, MD: American Society of Health-System
Pharmacists; 1998.
76. Catania PN, ed. King guide to parenteral admixtures.
St. Louis, MO: King Guide; 1999.
77. American Society of Health-System Pharmacists. ASHP
guidelines: minimum standard for home care pharma-
cies. Am J Health-Syst Pharm. 1999; 56:629–38.
78. Scheckelhoff DJ. Labeling of sterile products. In:
Principles of sterile product preparation. Bethesda,
MD: American Society of Health-System Pharmacists;
1995:105–9.
79. Davis NM. Optimal checking of pharmacy-prepared
sterile products. Hosp Pharm. 1996; 31:102. Editorial.
80. Schneider PJ. End-product evaluation. In: Principles of
sterile product preparation. Bethesda, MD: American
Society of Health-System Pharmacists; 1995:125–8.
81. Meyer GE, Novielli KA, Smith JE. Use of refractive
index measurement for quality assurance of pediat-
ric parenteral nutrition solutions. Am J Hosp Pharm.
1987; 44:1617–20.
82. Scheckelhoff DJ. Handling of sterile products outside
the pharmacy. In: Principles of sterile product prepa-
ration. Bethesda, MD: American Society of Health-
System Pharmacists; 1995:117–20.
83. Chamallas SN, Fishwick JJ, Riesenberg M. Special
delivery, keeping the product stable during shipping.
Infusion. 1997; 4(3):30–2.
84. McKinnon BT. Documentation of sterile product prep-
arations. In: Principles of sterile product preparation.
Bethesda, MD: American Society of Health-System
Pharmacists; 1995:129–31.
85. Schumock GT, Kafka PS, Tormo VJ. Design, construc-
tion, implementation, and cost of a hospital pharmacy
cleanroom. Am J Health-Syst Pharm. 1998; 55:458–63.
86. Gianino RR. Misconceptions about cleanrooms. Am J
Hosp Pharm. 1994; 51:239–40. Letter.
87. Fundamentals of a microbiological environmental mon-
itoring program. Technical report no. 13. Philadelphia:
Parenteral Drug Association; 1990.
88. Whyte W. In support of settle plates. PDA J Pharm Sci
Technol. 1996; 50:201–4.
89. Hyde HA. Origin of bacteria in the clean room and
their growth requirements. PDA J Pharm Sci Technol.
1998; 52:154–8.
90. American Society of Health-System Pharmacists. ASHP
guidelines on the safe use of automated compounding
devices for the preparation of parenteral nutrition ad-
mixtures. Am J Health-Syst Pharm. 2000; 57:1343–8.
91. Davis NM. Unprecedented procedural safeguards
needed with the use of automated iv compounders.
Hosp Pharm. 1992; 27:488. Editorial.
92. Murphy C. Ensuring accuracy in the use of automatic
compounders. Am J Hosp Pharm. 1993; 50:60. Letter.
93. Dickson LB, Somani SM, Herrmann G, et al.
Automated compounder for adding ingredients to
parenteral nutrient base solutions. Am J Hosp Pharm.
1993; 50:678–82.
94. Fishwick JJ, Murphy CC, Riesenberg MC, et al.
Weight-based accuracy of parenteral nutrient solutions
prepared with an automated compounder. Am J Health-
Syst Pharm. 1997; 54:678–9.
95. Johnson R, Coles BJ, Tribble DA. Accuracy of three
automated compounding systems determined by end-
product laboratory testing and comparison with manual
preparation. Am J Health-Syst Pharm. 1998; 55:1503–7.
96. Combeau D, Rey JB, Rieutord A, et al. Accuracy of
two filling systems for parenteral nutrient solutions.
Am J Health-Syst Pharm. 1998; 55:1606–10.
97. Boylan JC. Essential elements of quality control. Am J
Hosp Pharm. 1983; 40:1936–9.
98. McKinnon BT. Preparation and sterilization of batch
compounds. In: Principles of sterile product prepara-
tion. Bethesda, MD: American Society of Health-
System Pharmacists; 1995:71–7.
99. McKinnon BT. Batch preparation documentation. In:
Principles of sterile product preparation. Bethesda,
MD: American Society of Health-System Pharmacists;
1995:79–94.
100. Lima HA. Required documentation for home infu-
sion pharmacies—compounding records. Int J Pharm
Compd. 1998; 2:354–9.
101. Avis KE. Assuring the quality of pharmacy-
prepared sterile products. Pharmacopeial Forum.
1997; 23:3567–76.
102. Fontan JE, Arnaud P, Brion F. Laminar-airflow ceiling
in a hospital pharmacy cleanroom. Am J Health-Syst
Pharm. 1998; 55:182–3. Letter.
103. Chandler SW, Trissel LA, Wamsley LM, et al. Eval-
uation of air quality in a sterile-drug preparation area
with an electronic particle counter. Am J Hosp Pharm.
1993; 50:2330–4.
104. Schneider PJ. Environmental monitoring. In: Principles
of sterile product preparation. Bethesda, MD: American
Society of Health-System Pharmacists; 1995:45–8.

104 Drug Distribution and Control: Preparation and Handling–Guidelines
105. Bacterial endotoxins test (general tests and assays
chapter 85). In: The United States pharmacopeia, 24th
rev., and The national formulary, 19th ed. Rockville,
MD: The United States Pharmacopeial Convention;
1999:1829-31.
106. Roberts JH, Wilson JD. Technical report no. 26: steril-
izing filtration of liquids. PDA J Pharm Sci Technol.
1998; 52(suppl S1):1–31.
107. Akers MJ. Sterilization and depyrogenation: princi-
ples and methods. Int J Pharm Compd. 1999; 3:263–9.
108. Pyrogen test (general tests and assays chapter 151).
In: The United States pharmacopeia, 24th rev., and
The national formulary, 19th ed. Rockville, MD: The
United States Pharmacopeial Convention; 1999:1850–1.
109. Aspects of container/closure integrity. Technical infor-
mation bulletin no. 4. Philadelphia: Parenteral Drug
Association; 1983.
110. Neidich RL. Selection of containers and closure sys-
tems for injectable products. Am J Hosp Pharm. 1983;
40:1924–7.
111. Validation of steam sterilization cycles. Technical in-
formation bulletin no. 1. Philadelphia: Parenteral Drug
Association; 1978.
112. Turco S, ed. Sterile dosage forms: their preparation
and clinical application. Philadelphia: Lea & Febiger;
1994:57–78.
113. McKinnon BT, Avis KE. Membrane filtration of pharma-
ceutical solutions. Am J Hosp Pharm. 1993; 50: 1921–36.
114. Eudailey WA. Membrane filters and membrane fil-
tration processes for health care. Am J Hosp Pharm.
1983; 40:1921–3.
115. Wilson JD. Aseptic process monitoring—a better strat-
egy. PDA J Pharm Sci Technol. 1999; 53:111–4.
116. Sterility tests (general tests and assays chapter 71). In:
The United States pharmacopeia, 24th rev., and The
national formulary, 19th ed. Rockville, MD: The United
States Pharmacopeial Convention; 1999:1818–23.
117. Choy FN, Lamy PP, Burkhart VD, et al. Sterility-testing
program for antibiotics and other intravenous admix-
tures. Am J Hosp Pharm. 1982; 39:452–6.
118. Doss HL, James JD, Killough DM, et al. Microbiologic
quality assurance for intravenous admixtures in a small
hospital. Am J Hosp Pharm. 1982; 39:832–5.
119. Posey LM, Nutt RE, Thompson PD. Comparison of two
methods for detecting microbial contamination in intra-
venous fluids. Am J Hosp Pharm. 1981; 38:659–62.
120. Akers MJ. Progress toward a preferred method of
monitoring the sterility of intravenous admixtures. Am
J Hosp Pharm. 1982; 39:1297. Editorial.
121. Hoffman KH, Smith FM, Godwin HN, et al. Evaluation
of three methods for detecting bacterial contamination
in intravenous solutions. Am J Hosp Pharm. 1982;
39:1299–302.
122. Miller CM, Furtado D, Smith FM, et al. Evaluation
of three methods for detecting low-level bacterial
contamination in intravenous solutions. Am J Hosp
Pharm. 1982; 39:1302–5.
123. DeChant RL, Furtado D, Smith FH, et al. Determining
a time frame for sterility testing of intravenous admix-
tures. Am J Hosp Pharm. 1982; 39:1305–8.
124. Bronson MH, Stennett DJ, Egging PK. Sterility testing
of home and inpatient parenteral nutrition solutions.
JPEN J Parenter Enteral Nutr. 1988; 12:25–8.
125. Levchuk JW, Nolly RJ, Lander N. Method for testing
the sterility of total nutrient admixtures. Am J Hosp
Pharm. 1988; 45:1311–21.
126. Akers MJ, Wright GE, Carlson KA. Sterility testing of
antimicrobial-containing injectable solutions prepared
in the pharmacy. Am J Hosp Pharm. 1991; 48:2414-8.
127. Murray PR, Sandrock MJ. Sterility testing of a total
nutrient admixture with a biphasic blood-culture sys-
tem. Am J Hosp Pharm. 1991; 48:2419–21.
a
Unless otherwise stated in this document, the term sterile products
refers to sterile drugs or nutritional substances that are prepared
(e.g., compounded or repackaged) by pharmacy personnel.
b
Ampuls, swabbed and opened appropriately with contents filtered
upon removal, should be considered part of a “closed” system.
c
Isolator guidelines appear under risk level 1 sections because their
greatest use is likely to be in the preparation of cytotoxic sterile
products, most of which are risk level 1 processes.
d
The need to alternate germicides is controversial. According to Akers
and Moore (Microbiological monitoring of pharmaceutical clean-
rooms: the need for pragmatism, J Adv Appl Contam Control. 1998;
1[1]:23-4,26,28,30), the data do not support alternating germicides. A
literature search (Kopis EM. Cleanrooms. 1996; 10[10]:48-v50) found
little evidence for periodic alternation of disinfectants; the search did
find that alternating use of acidic and alkaline phenolic disinfectants
reduces resistance arising in pseudomonads adhering to hard surfaces.
If ethanol 70% or isopropyl alcohol 70% is used as the primary disin-
fectant, it should be sterile filtered through a 0.22-μm filter before use.
e
According to Trissel and Chandler (Am J Hosp Pharm. 1993;
50:1858–61), pharmacy air is nearly class 10,000 cleanroom quality
already. However, true cleanrooms add HEPA air filtering and des-
ignate room air changes and room air pressure differentials to ensure
cleanliness (Am J Hosp Pharm. 1994; 51:239-40. Letter).
f
Note that the International Organization for Sanitation (ISO) is prepar-
ing documents that should replace Federal Standard 209E. The ISO
documents (numbered 14644-1 through 14644-7 and 14698-1 through
14698-3) are being prepared by a technical committee consisting of
members from six countries, including the United States. Document
14644-1 is published in final form and classifies the air cleanliness of
cleanrooms and associated controlled environments. In 14644-1 ISO
cleanroom class 5 is equivalent to Federal Standard 209E class 100,
and ISO class 7 is equivalent to Federal Standard 209E class 10,000.
g
As in general information chapter 1206 in USP, which does not re-
quire sterility testing until the third risk level, this assumes that ster-
ile components remain sterile throughout preparation. Many sterile
products are prepared in batches too small or used too quickly after
preparation to make sterility testing meaningful. Also, one of the
purposes of process validation is to determine that personnel and
processes can produce a sterile product.
Supersedes the ASHP Technical Assistance Bulletin on Quality
Assurance for Pharmacy-Prepared Sterile Products, dated
September 24, 1993.
Approved by the ASHP Board of Directors, on April 27, 2000
Developed through the ASHP Council on Professional Affairs.
Copyright © 2000, American Society of Health-System Pharmacists,
Inc. All rights reserved.
The bibliographic citation for this document is as follows: American
Society of Health-System Pharmacists. ASHP Guidelines on Quality

Drug Distribution and Control: Preparation and Handling–Guidelines 105
Assurance for Pharmacy-Prepared Sterile Products. Am J Health-
Syst Pharm. 2000; 57:1150–69.
Appendix A—Glossary
Action Level: Established particulate or microbial counts or
results that require corrective action when exceeded.
Aseptic Preparation or Aseptic Processing: The technique
involving procedures designed to preclude contamina-
tion (of drugs, packaging, equipment, or supplies) by
microorganisms during processing.
Batch Preparation: Compounding of multiple sterile prod-
uct units, in a single discrete process, by the same in-
dividuals, carried out during one limited time period.
Cleanroom: A room (1) in which the concentration of air-
borne particles is controlled, (2) that is constructed and
used in a manner to minimize the introduction, genera-
tion, and retention of particles inside the room, and (3)
in which other relevant variables (e.g., temperature,
humidity, and pressure) are controlled as necessary.
28
For example, the air particle count in a class 100 clean-
room cannot exceed a total of 100 particles 0.5 μm or
larger per cubic foot of air.
29
Clean Zone: Dedicated space (1) in which the concentration
of airborne particles is controlled, (2) that is constructed
and used in a manner that minimizes the introduction,
generation, and retention of particles inside the zone,
and (3) in which other relevant variables (e.g., tempera-
ture, humidity, and pressure) are controlled as necessary.
This zone may be open or enclosed and may or may not
be located within a cleanroom.
28
For example, an open-
architecture controlled area should be a clean zone.
Closed-System Transfer: The movement of sterile products
from one container to another in which the contain-
ers-closure system and transfer devices remain intact
throughout the entire transfer process, compromised
only by the penetration of a sterile, pyrogen-free nee-
dle or cannula through a designated closure or port to
effect transfer, withdrawal, or delivery. Withdrawal of
a sterile solution from an ampul through a particulate
filter in a class 100 environment would generally be
considered acceptable; however, the use of a flexible
closure vial, when available, would be preferable.
Compounding: For purposes of these guidelines, com-
pounding simply means the mixing of ingredients
to prepare a medication for patient use. This activity
would include dilution, admixture, repackaging, re-
constitution, and other manipulations of sterile prod-
ucts.
Controlled Area: For purposes of these guidelines, a controlled
area is the area designated for preparing sterile products.
This is referred to as the buffer zone (i.e., the cleanroom in
which the laminar-airflow workbench is located) by USP.
15
Corrective Action: Action to be taken when the results of
monitoring indicate a loss of control or when action
levels are exceeded.
Critical Area: Any area in the controlled area where prod-
ucts or containers are exposed to the environment.
Critical Site: An opening providing a direct pathway between
a sterile product and the environment or any surface
coming into contact with the product or environment.
Critical Surface: Any surface that comes into contact with
previously sterilized products or containers.
Designated Pharmacist: The pharmacist chosen by experi-
ence and training to be in charge of a sterile product
preparation area or unit in a licensed pharmacy.
Expiration Date: The date (and time, when applicable)
beyond which a product should not be used (i.e., the
product should be discarded beyond this date and
time). Expiration date and time should be assigned on
the basis of both stability and risk level, whichever is
the shorter period. Note: Circumstances may occur in
which the expiration date and time arrive while an infu-
sion is in progress. When this occurs, judgment should
be applied in determining whether it is appropriate
to discontinue that infusion and replace the product.
Organizational policies on this should be clear.
15
High-Efficiency Particulate Air (HEPA) Filter: A filter
composed of pleats of filter medium separated by rigid
sheets of corrugated paper or aluminum foil that direct
the flow of air forced through the filter in a uniform par-
allel flow. HEPA filters remove 99.97% of all air par-
ticles 0.3 μm or larger. When HEPA filters are used as a
component of a horizontal- or vertical-laminar-airflow
workbench, an environment can be created consistent
with standards for a class 100 cleanroom.
Isolator (or Barrier Isolator): A closed system made up
of four solid walls, an air-handling system, and trans-
fer and interaction devices. The walls are constructed
so as to provide surfaces that are cleanable with cov-
ing between wall junctures. The air-handling system
provides HEPA filtration of both inlet and exhaust
air. Transfer of materials is accomplished through air
locks, glove rings, or ports. Transfers are designed to
minimize the entry of contamination. Manipulations
can take place through either glove ports or half-suits.
Media Fill: See process validation or simulation.
Preservatives: For purposes of these guidelines, preserva-
tives refer to any additive intended to extend the con-
tent, stability, or sterility of active ingredients (e.g., an-
tioxidants, emulsifiers, bacteriocides).
Process Validation or Simulation: Microbiological simulation
of an aseptic process with growth medium processed in a
manner similar to the processing of the product and with
the same container or closure system.
30
Process simula-
tion tests are synonymous with medium fills, simulated
product fills, broth trials, and broth fills.
Quality Assurance: For purposes of these guidelines, quality
assurance is the set of activities used to ensure that the pro-
cesses used in the preparation of sterile drug products lead
to products that meet predetermined standards of quality.
Quality Control: For purposes of these guidelines, quality con-
trol is the set of testing activities used to determine that the
ingredients, components (e.g., containers), and final sterile
products prepared meet predetermined requirements with
respect to identity, purity, nonpyrogenicity, and sterility.
Repackaging: The subdivision or transfer of a compounded
product from one container or device to a different con-
tainer or device, such as a syringe or an ophthalmic con-
tainer.
Sterilization: A validated process used to render a product
free of viable organisms.
Sterilizing Filter: A filter that, when challenged with a solution
containing the microorganism Pseudomonas diminuta at
a minimum concentration of 10
12
organisms per square
centimeter of filter surface, will produce a sterile effluent.

106 Drug Distribution and Control: Preparation and Handling–Guidelines
Temperatures (USP): Frozen means temperatures between
–20 and –10 °C (–4 and 14 °F). Refrigerated means
temperatures between 2 and 8°C (36 and 46 °F). Room
temperature means temperatures between 15 and 30 °C
(59 and 86 °F).
Validation: Documented evidence providing a high degree
of assurance that a specific process will consistently
produce a product meeting its predetermined specifi-
cations and quality attributes.
Worst Case: A set of conditions encompassing upper and
lower processing limits and circumstances, including
those within standard operating procedures, that pose
the greatest chance of process or product failure when
compared with ideal conditions. Such conditions do
not necessarily induce product or process failure.
31
Appendix B—Comparison
of Risk-Level Attributes
This appendix does not show all details of the guidelines,
nor does it tell whether an aspect of the sterile compound-
ing process is “required” (must be) or “advisable” (should
be). Regardless of the examples given, each compounding
pharmacist must decide, according to the circumstances at
the time, what conditions are appropriate for compounding
a sterile product. In an emergency, it may be of more benefit
to a patient to receive a sterile drug prepared under lower
risk-level conditions. For the immunocompromised patient,
even simple, single-patient admixtures may need to be com-
pounded under higher risk-level conditions.
Definition of Products by Risk Level
Risk Level 1
Risk Level 2
Products that are (1) stored at room
temperature and completely
administered within 28 hours from
preparation, (2) unpreserved and
sterile and prepared for administration
to one patient, or batch prepared for
administration to more than one patient
and contain suitable preservatives, and
(3) prepared by closed-system aseptic
transfer of sterile, nonpyrogenic,
finished pharmaceuticals obtained
from licensed manufacturers into
sterile final containers obtained from
licensed manufacturers.
Products that are (1) administered
beyond 28 hours after preparation
and storage at room temperature,
(2) batch prepared without
preservatives and intended for use
by more than one patient, or (3)
compounded by complex or numerous
manipulations of sterile ingredients
obtained from licensed manufacturers
in a sterile container obtained from
a licensed manufacturer by using
closed-system, aseptic transfer.
Risk Level 3
Products that are (1) compounded
from nonsterile ingredients or with
nonsterile components, containers, or
equipment before terminal sterilization
or (2) prepared by combining multiple
ingredients (sterile or nonsterile) by
using an open-system transfer or open
reservoir before terminal sterilization.
Examples of Sterile Products by Risk Level
Risk Level 1
Risk Level 2 Risk Level 3
Single-patient admixture
Injections for use in portable pump
or reservoir over multiple days
Alum bladder irrigation
Policies and Procedures
Risk Level 1
Risk Level 2
Up-to-date policies and procedures for compounding
sterile products should be available to all involved
personnel. When policies are changed, they
should be updated. Procedures should address
personnel education and training, competency
evaluation, product acquisition, storage and
handling of products and supplies, storage and
delivery of final products, use and maintenance
of facilities and equipment, appropriate garb and
conduct of personnel working in the controlled area,
process validation, preparation technique, labeling,
documentation, quality control, and material
movement.
Risk Level 3
In addition to risk level 1
guidelines, procedures describe
environmental monitoring devices
and techniques, cleaning
materials and disinfectants,
equipment accuracy monitoring,
limits of acceptability
and corrective actions for
environmental monitoring and
process validation, master
formula and work sheets,
personnel garb, lot numbers, and
other quality control methods.
Procedures cover every aspect
of preparation of level 3 sterile
products, so that all products
have the identity, strength,
quality, and purity purported for
the product. Thirteen general
policies and procedures, in
addition to those in levels 1 and
2, are required.
Single-patient ophthalmic, preserved
Single-patient syringes without preservatives
used in 28 hours
Batch-prefilled syringes with preservatives
Total parenteral nutrient (TPN) solution made
by gravity transfer of carbohydrate and
amino acids into an empty container with the
addition of sterile additives with a syringe and
needle
Autoclaved i.v. solutions
Batch-reconstituted antibiotics
without preservatives
Batch-prefilled syringes without
preservatives
TPN solutions mixed with an
automatic compounding device
Morphine injection made from powder or
tablets
TPN solutions made from dry amino acids
TPN solutions sterilized by final filtration
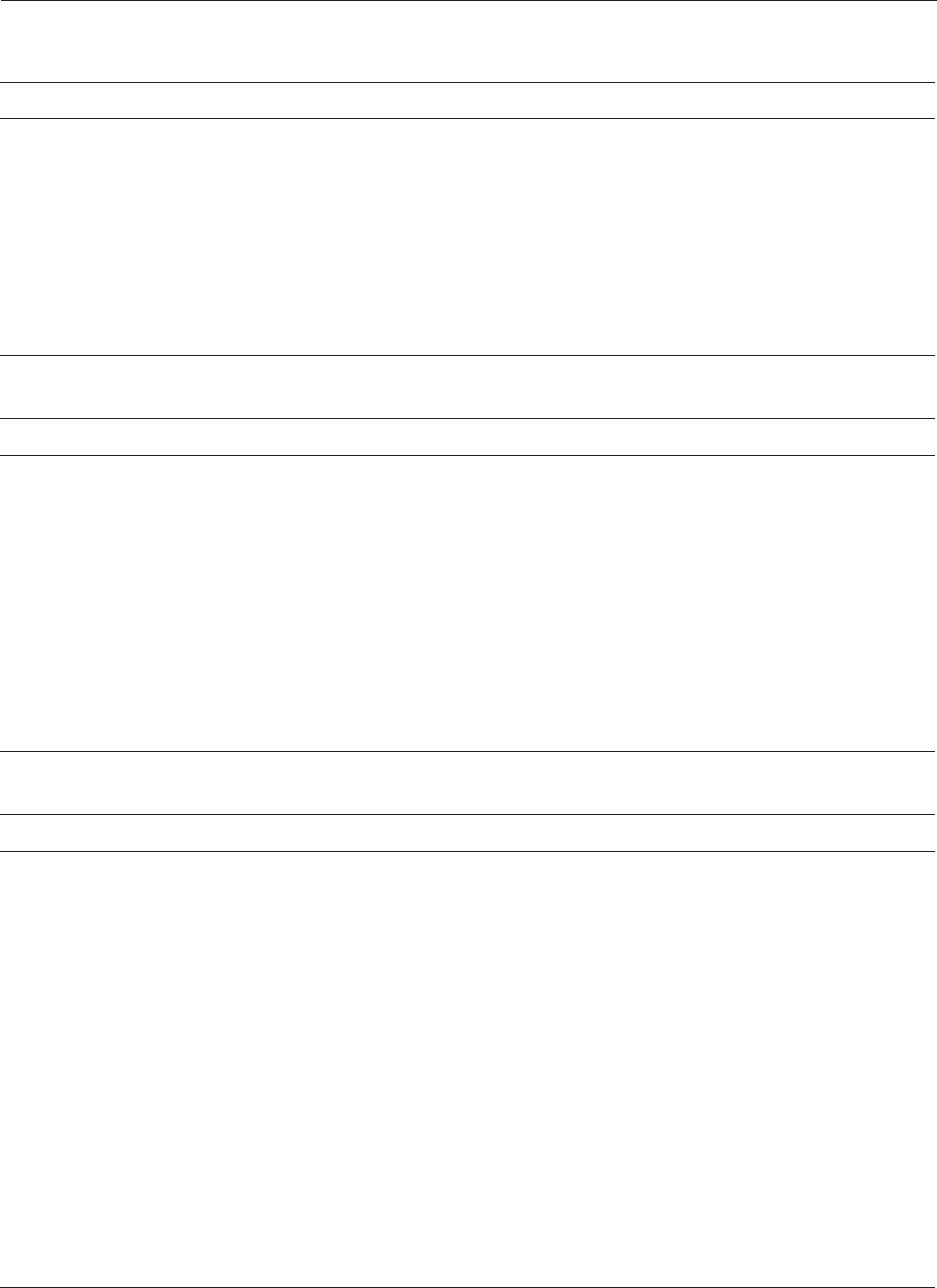
Drug Distribution and Control: Preparation and Handling–Guidelines 107
Personnel Education, Training, and Evaluation
Risk Level 1 Risk Level 2
All pharmacy personnel preparing
sterile products should receive
suitable didactic and experiential
training and competency evaluation
through demonstration or testing
(written or practical). In addition
to the policies and procedures
listed above, education includes
chemical, pharmaceutical, and clinical
properties of drugs and current good
compounding practices.
Risk Level 3
Operators have specific education,
training, and experience to
prepare risk level 3 products.
Pharmacist knows principles of
good compounding practice for risk
level 3 products, including aseptic
processing; quality assurance of
environmental, component, and
end-product testing; sterilization;
and selection and use of containers,
equipment, and closures.
In addition to guidelines in risk level
1, training includes assessment of
competency in all types of risk level
2 procedures via process simulation.
Personnel show competency in end-
product testing as well.
Storage and Handling in the Pharmacy
Risk Level 1
Solutions, drugs, supplies, and equipment must be stored
according to manufacturer or USP requirements. Refrigerator
and freezer temperatures should be documented daily. Other
storage areas should be inspected regularly to ensure that
temperature, light, moisture, and ventilation meet requirements.
Drugs and supplies should be shelved above the floor. Expired
products must be removed from active product storage
areas. Personnel traffic in storage areas should be minimized.
Removal of products from boxes should be done outside
controlled areas. Disposal of used supplies should be done at
least daily. Product-recall procedures must permit retrieving
affected products from specific involved patients.
Risk Level 2
All guidelines for risk level
1 apply.
Risk Level 3
In addition to risk level 1
guidelines, procedures
include procurement,
identification, storage,
handling, testing, and
recall of components
and finished products.
Finished but untested
products must be
quarantined under
minimal risk for
contamination or loss of
identity in an identified
quarantine area.
Risk Level 3
Products must be prepared in a
class 100 workbench in a class
10,000 cleanroom, in a class 100
cleanroom, or in a suitable barrier
isolator. Access to the cleanroom
must be limited to those preparing
the products who are in appropriate
garb. Methods are needed for
cleaning, preparing, sterilizing,
calibrating, and documenting the use
of all equipment. Walls and ceilings
should be disinfected weekly. All
nonsterile equipment that is to come
in contact with the sterilized final
product should be sterilized before
introduction into the cleanroom. An
anteroom of high cleanliness (i.e.,
class 100,000) should be provided.
Appropriate cleaning and disinfection
of the environment and equipment
are required.
Risk Level 2
In addition to risk level 1
guidelines, the following are
recommended for risk level
2 products: controlled area
must meet class 10,000
cleanroom standards; cleaning
supplies should be selected
to meet cleanroom standards;
critical-area work surface
must be cleaned between
batches; floors should be
disinfected daily, equipment
surfaces weekly, and walls
monthly; and there should be
environmental monitoring of air
and surfaces. An anteroom of
high cleanliness is desirable.
Automated compounding
devices must be calibrated
and verified as to accuracy,
according to procedure.
Risk Level 1
The controlled area should be separated from
other operations to minimize unnecessary
flow of materials and personnel through
the area. The controlled area must be
clean, well lighted, and of sufficient size for
sterile compounding. A sink with hot and
cold water should be near, but not in, the
controlled area. The controlled area and
inside equipment must be cleaned and
disinfected regularly. Sterile products must
be prepared in a class 100 environment (the
critical area), such as within a horizontal- or
vertical-laminar-airflow workbench or barrier
isolator. Computer entry, order processing,
label generation, and record keeping should
be performed outside the critical area. The
critical area must be disinfected periodically.
A workbench should be recertified every six
months or when it is moved; prefilters should
be changed periodically. Pumps should be
recalibrated according to procedure.
Facilities and Equipment

108 Drug Distribution and Control: Preparation and Handling–Guidelines
Garb
Risk Level 1
In the controlled area, personnel wear low-
particulate, clean clothing covers such as
clean gowns or coverall with sleeves having
elastic cuffs. Hand, finger, and wrist jewelry
is minimized or eliminated. Nails are clean
and trimmed. Gloves are recommended;
those allergic to latex rubber must wear
gloves made of a suitable alternative.
Head and facial hair is covered. Masks are
recommended during aseptic preparation.
Personnel preparing sterile products scrub
their hands and arms with an appropriate
antimicrobial skin cleanser.
Risk Level 2
In addition to risk level 1
guidelines, gloves, gowns, and
masks are required. During
sterile preparation, gloves
should be rinsed frequently
with a suitable agent (e.g.,
70% isopropyl alcohol) and
changed when their integrity
is compromised. Shoe covers
are helpful in maintaining the
cleanliness of the controlled
area.
Risk Level 3
In addition to risk level 1 and 2
guidelines, cleanroom garb must
be worn inside the controlled area
at all times during the preparation
of risk level 3 sterile products. Attire
consists of a low-shedding coverall,
head cover, face mask, and shoe
covers. Before donning this garb,
personnel must thoroughly wash
their hands and arms. Upon return to
the controlled area or support area
during processing, personnel should
regown with clean garb.
Aseptic Technique and Product Preparation
Risk Level 1
Risk Level 2
Risk Level 3
In addition to risk level 1 and
2 guidelines, nonsterile
components must meet
USP standards for identity,
purity, and endotoxin levels,
as verified by a pharmacist.
Batch master work sheets
should also include
comparisons of actual
with anticipated yields,
sterilization methods, and
quarantine specifications.
Presterilized containers
should be used if feasible.
Final containers must
be sterile and capable
of maintaining product
integrity throughout shelf
life. Sterilization method
is based on properties of
the product. Final filtration
methods require attention to
many elements of product,
filter, and filter integrity.
In addition to risk level 1
guidelines, a master
work sheet containing
formula, components,
procedures, sample label,
final evaluation, and testing
is made for each product
batch. A separate work
sheet and lot number are
used for each batch. When
combining multiple sterile
ingredients, a second
pharmacist should verify
calculations. The pharmacist
should verify data
entered into an automatic
compounder before
processing and check the
end product for accuracy.
Sterile products must be prepared in a class 100
environment. Personnel scrub their hands and forearms
for an appropriate period at the beginning of each aseptic
compounding process. Eating, drinking, and smoking are
prohibited in the controlled area. Talking is minimized to
reduce airborne particles. Ingredients are determined to
be stable, compatible, and appropriate for the product to
be prepared, according to manufacturer, USP, or scientific
references.
Ingredients result in final products that meet
physiological norms as to osmolality and pH for the
intended route of administration. Ingredients and
containers are inspected for defects, expiration, and
integrity before use. Only materials essential for aseptic
compounding are placed in the workbench. Surfaces
of ampuls and vials are disinfected before placement
in the workbench. Sterile components are arranged in
the workbench to allow uninterrupted laminar airflow
over critical surfaces of needles, vials, ampuls, etc.
Usually only one person and one preparation are in the
workbench at a time. Automated devices and equipment
are cleaned, disinfected, and placed in the workbench
to enable laminar airflow. Aseptic technique is used to
avoid touch contamination of critical sites of containers
and ingredients. Sterile powders are completely
reconstituted. Particles are filtered from solutions. Needle
cores are avoided. The pharmacist checks before,
during, and after preparation to verify the identity and
amount of ingredients before release.
Process Validation
Risk Level 1 Risk Level 2
All persons who prepare sterile products should pass a
process validation of their aseptic technique before
they prepare sterile products for patient use. Personnel
competency should be reevaluated by process validation
at least annually, whenever the quality assurance
program yields an unacceptable result, and whenever
unacceptable techniques are observed. If microbial
growth is detected, the entire sterile process must be
evaluated, corrective action taken, and the process
simulation test performed again.
All risk level 1 guidelines apply,
and process-simulation
procedures should cover
all types of manipulations,
products, and batch sizes
that are encountered in risk
level 2.
Risk Level 3
In addition to risk level 1 and 2
guidelines, written policies
should be made to validate
all processes (including all
procedures, components,
equipment, and techniques)
for each risk level 3 product.

Drug Distribution and Control: Preparation and Handling–Guidelines 109
Handling Sterile Products Outside the Pharmacy
Risk Level 1
Sterile products are transported so as to be protected from excesses of
temperatures and light. Transit time and condition should be specified.
Delivery personnel should be trained as appropriate. Pharmacists ascertain
that the end user knows how to properly store products. End users notify
pharmacists when storage conditions are exceeded or when products
expire so that pharmacists can arrange safe disposal or return.
Risk Level 2
All guidelines for risk
level 1 should be
met.
Risk Level 3
All guidelines for risk
level 1 should be
met.
Documentation
Risk Level 1 Risk Level 2
The following must be documented according
to policy, laws, and regulations: (1) training
and competency evaluation of employees,
(2) refrigerator and freezer temperature logs,
(3) certification of workbenches, and (4) other
facility quality control logs as appropriate.
Pharmacists maintain appropriate records for the
compounding and dispensing of sterile products.
In addition to the guidelines in
risk level 1, documentation
of end-product testing and
batch-preparation records
must be maintained
according to policies,
laws, and regulations.
Risk Level 3
In addition to the guidelines in risk
levels 1 and 2, documentation
for risk level 3 products must
include (1) preparation work sheet,
(2) sterilization records if applicable,
(3) quarantine records if applicable,
and (4) end-product evaluation and
testing records.
Risk Level 3
In addition to risk level 1 and 2
guidelines, there must be a reliable
method for establishing all expiration
dates, including laboratory testing of
product stability, pyrogenicity, and
chemical content when necessary.
Risk Level 2
All guidelines for risk level
1 should be met.
Risk Level 1
Expiration Dating
All sterile products must bear an appropriate expiration
date. Expiration dates are assigned based on
current drug stability information and sterility
considerations. The pharmacist considers all
aspects of the final product, including drug reservoir,
drug concentration, and storage conditions.
Labeling
Risk Level 1
Sterile products should be labeled with at least the following information: (1) for
patient-specific product’s, the patient’s name and other appropriate patient
identification; for batch-prepared products, control or lot numbers, (2) all solution
and ingredient names, amounts, strengths, and concentrations, (3) expiration date
(and time when applicable), (4) prescribed administration regimen, (5) appropriate
auxiliary labeling, (6) storage requirements, (7) identification of the responsible
pharmacist, (8) any device-specific instructions, and (9) any additional information,
in accordance with state and federal regulations. A reference number for the
prescription or order may also be helpful. The label should be legible and affixed to
the product so that it can be read while being administered.
Risk Level 2
All guidelines
for risk level 1
must be met.
Risk Level 3
All guidelines for
risk levels 1
and 2 must be
met.
Risk Level 3
In addition to risk level 1 and 2 guidelines, the medium-fill
procedure should be supplemented with a program
of end-product sterility testing according to a formal
sampling plan. Samples should be statistically
adequate to reasonably ensure that batches are sterile.
A method for recalling batch products should be
established if end-product testing yields unacceptable
results. Each sterile preparation or batch must be
laboratory tested for conformity to written specifications
(e.g., concentration, pyrogenicity). It is advisable to
quarantine sterile products compounded from nonsterile
components pending the results of end-product testing.
Risk Level 2
In addition to risk level 1
guidelines, toxic products,
like concentrated glucose
and potassium chloride,
should be tested for
accuracy of concentration.
End-Product Evaluation
Risk Level 1
The final product must be
inspected for container leaks,
integrity, solution cloudiness or
phase separation, particulates
in solution, appropriate
solution color, and solution
volume. The pharmacist must
verify that the product was
compounded accurately as
to ingredients, quantities,
containers, and reservoirs.
